34 Open Rhinoplasty
Introduction
Open rhinoplasty is not a new operation. Around 600 BC, the Sushruta Ayurveda described external nasal surgery being performed in India. 1 Photos documenting Joseph’s first published reduction rhinoplasty case are often shown in profile view. Sometimes overlooked, though, is the full-length dorsal incision that was utilized for his approach. 1 In 1920, Gillies degloved the nasal tip using an “elephant trunk incision” placed in the inferior columella. The modern era of open rhinoplasty began in 1934 with Rethi’s description of a high transcolumellar incision to expose the tip alone. 2 Sercer, in Zagreb, Yugoslavia, performed nasal decortication by extending the exposure to include the entire nasal pyramid in 1956. 3 Padovan, a student of Sercer, further utilized this external exposure to perform a septoplasty. 4 The era of open rhinoplasty in North America was ushered in by his presentation of this technique at the First International Symposium of the American Academy of Facial Plastic and Reconstructive Surgery in 1970. The technique has since stirred controversy, and until the last 20 years it was promoted mainly by a handful of advocates. Goodman, of Toronto, 5 , 6 is generally recognized as the first North American to embrace the technique, followed by Anderson, Johnson, 7 Wright, 8 and others. Today, open rhinoplasty has achieved a respected position among rhinoplasty techniques and has become the one most commonly practiced by facial plastic surgeons. 9 , 10 Teaching of this technique in residency and postgraduate programs is ubiquitous. 11 Now, almost 70 years since its modern day origins in Europe, renewed interest in the technique is being seen there as well.
Indications
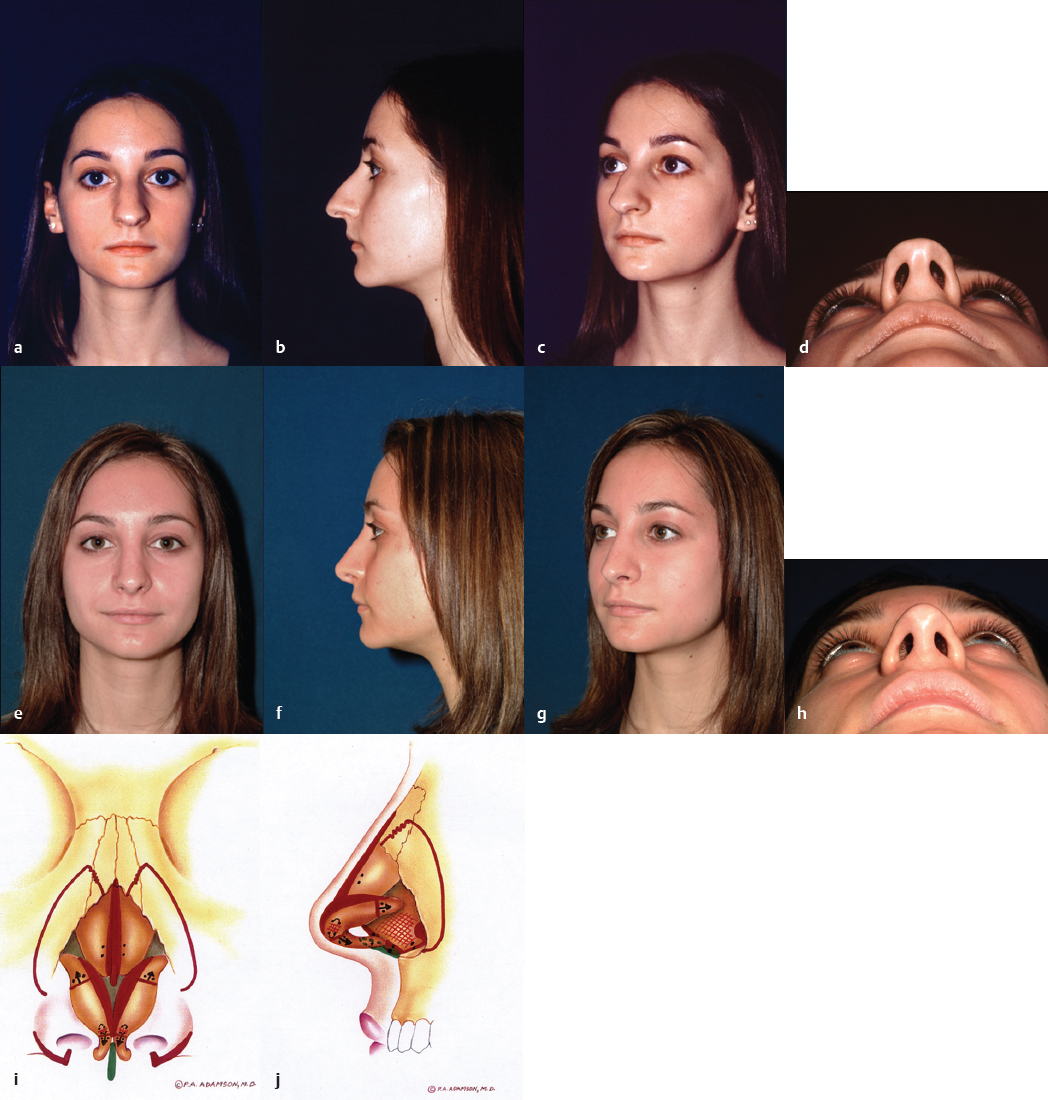
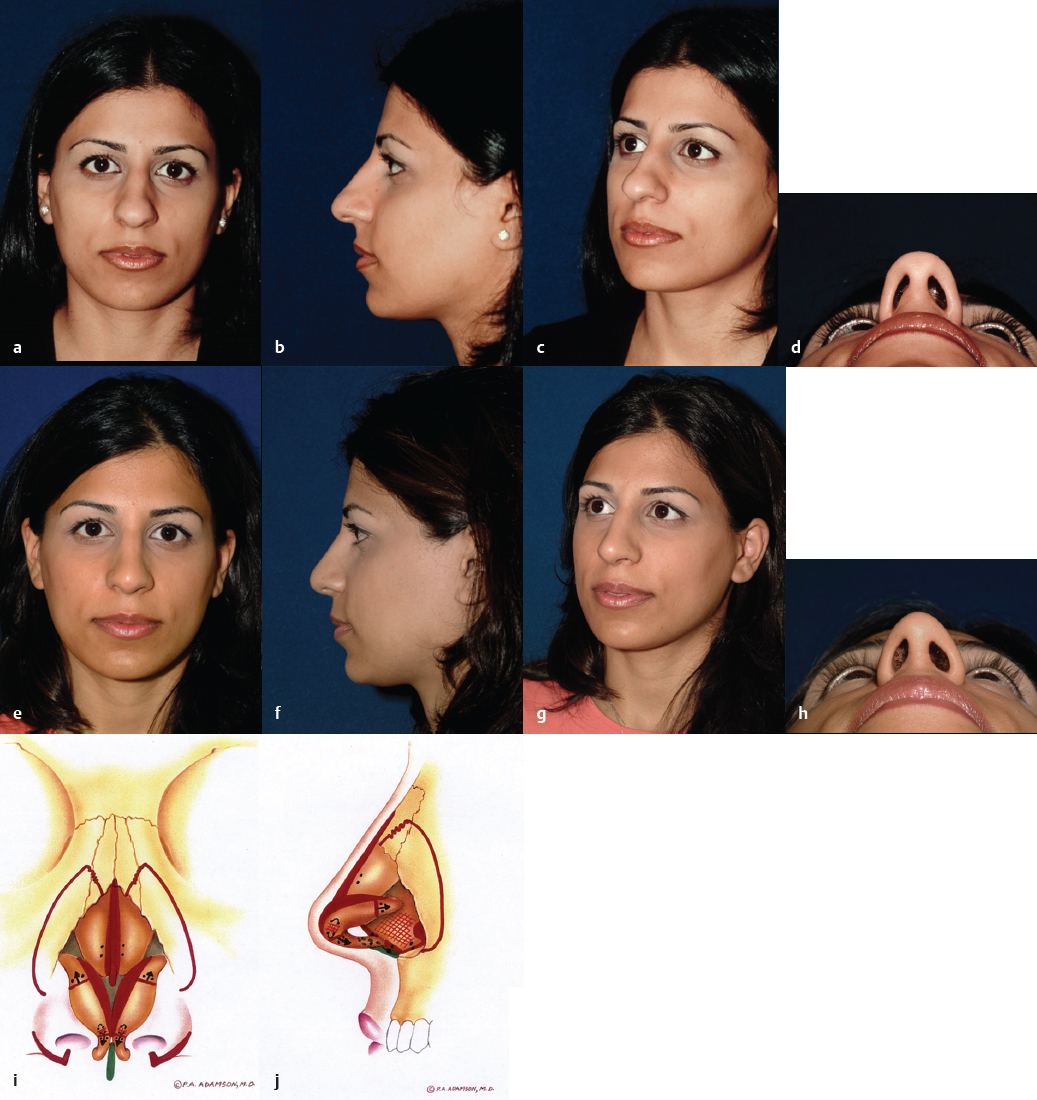
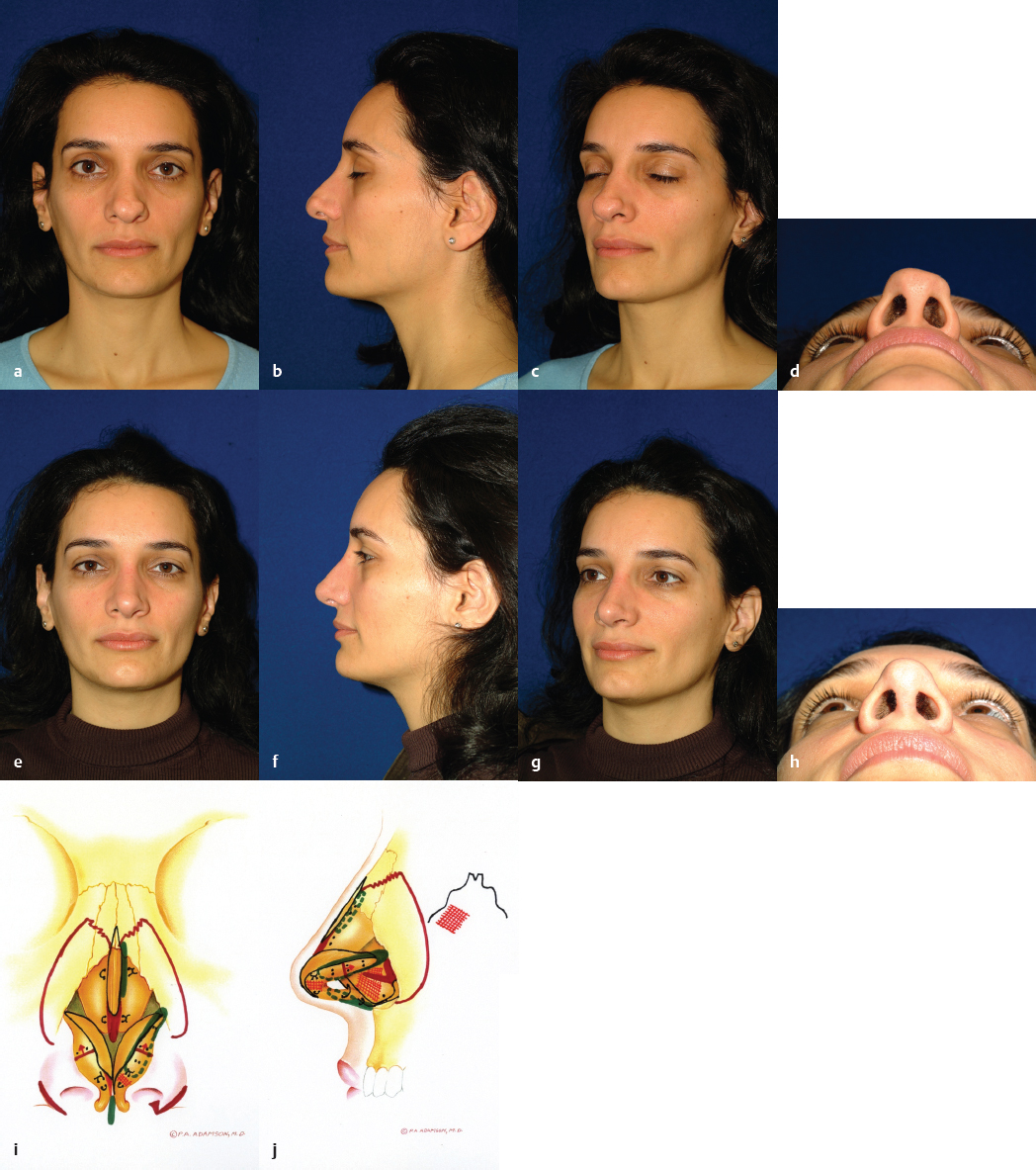
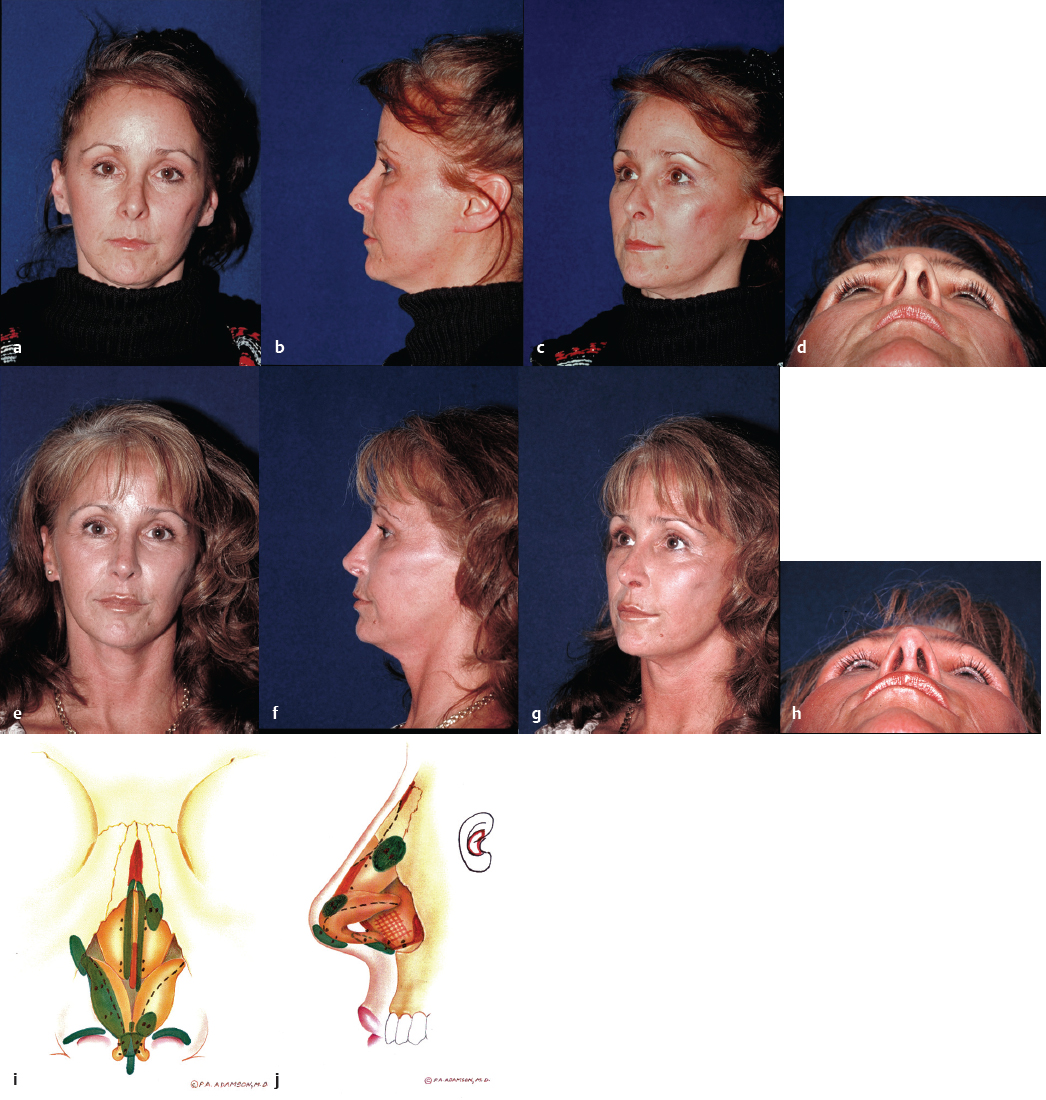
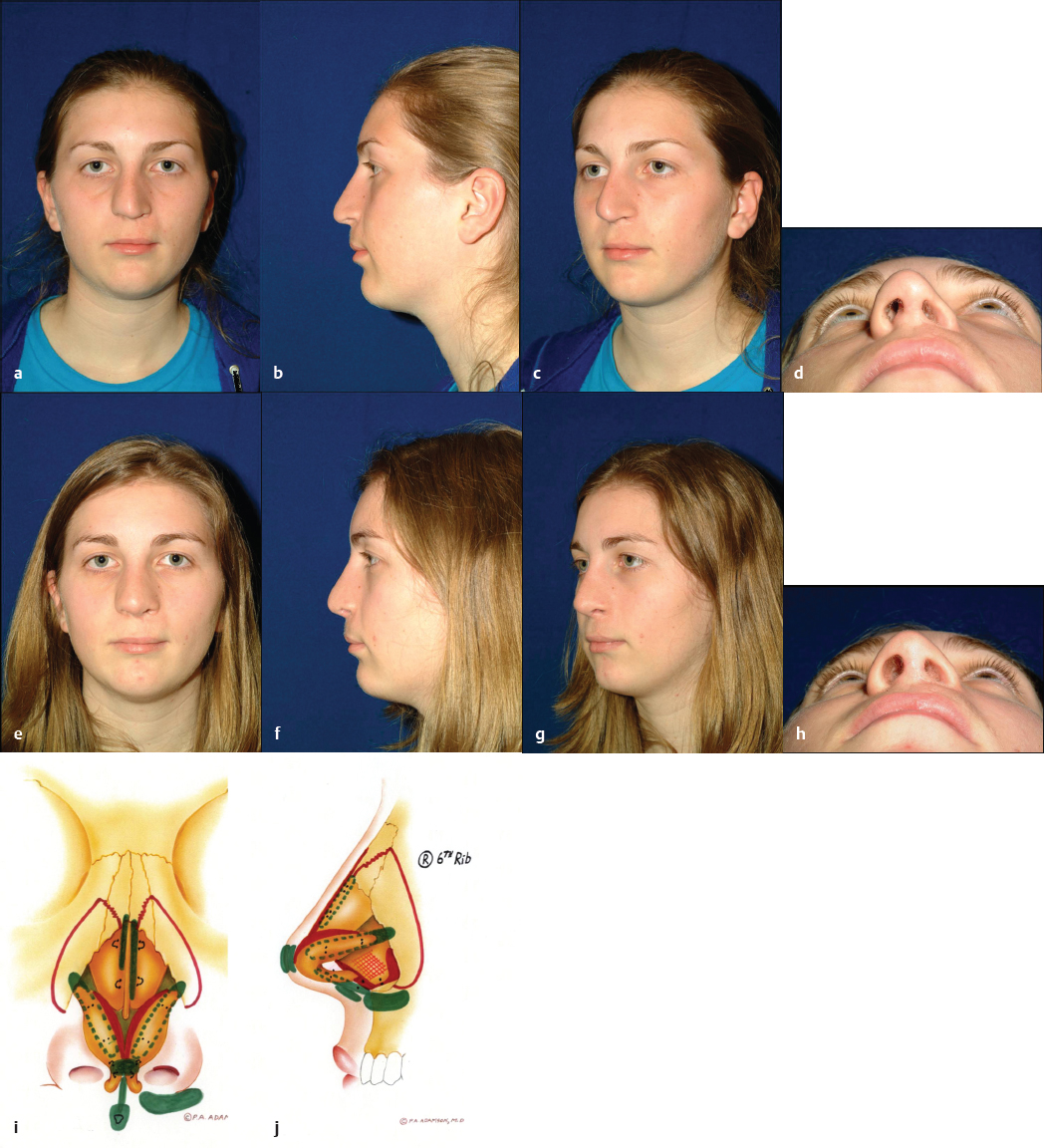
It is recognized that each rhinoplasty surgeon has a varied surgical experience and therefore will have unique indications for the open technique. In years past, the approach was grudgingly supported for difficult or revision cases. However, indications have expanded commensurate with widespread increasing levels of comfort and familiarity with this technique. In our experience, open rhinoplasty is the technique of choice for all cases unless a comparable improvement for a definable deformity can be obtained with the closed approach. The open approach offers clear diagnostic and therapeutic advantages for many challenging functional and cosmetic nasal deformities, primarily resulting from the broad undistorted exposure it affords. This is especially true with respect to the premaxillary spine, caudal septum, dorsal and superior septum, lobule, and superior dorsum. An unparalleled diagnosis of the underlying anatomy resulting in the external deformity can be made via the open approach. Sutures can be placed, grafts exactly trimmed, and asymmetries corrected without distortion of surrounding tissues. Scar tissue and redundant subcutaneous tissue are more easily excised. The valve region can be well protected, and the absence of incisions in the intercartilaginous region diminishes subsequent obstructive phenomena by precluding scar formation and disruption of one of the tip support mechanisms. A majority of facial plastic surgeons in North America now relies on this technique to achieve consistently good and reproducible results for a wide variety of indications ( Figs. 34.1–34.7 ).


Preoperative Evaluation
At the initial consultation, a complete history and examination is performed with specific emphasis placed on functional and aesthetic nasal diagnosis. The patient’s wishes are determined and standard photographs are reviewed to clarify the surgical goals. Patient education regarding realistic expectations and the possibility of minor postoperative asymmetries are underscored. Surgical protocols and risks are outlined. Referral for further investigations, including nasal airflow studies, imaging, and allergy testing, may be warranted, as mucosal disorders are optimally treated preoperatively. We routinely review details of the surgical plan with the patient at a second sitting along with any relevant test results. A rhinoplasty assessment sheet is completed, and a detailed written surgical plan is formulated for each patient.
Anesthesia
Most rhinoplasty patients are treated on an outpatient basis using general or neuroleptic anesthesia with an anesthesiologist in attendance. Amoxicillin (2 g) is given intravenously for bacterial prophylaxis. We do not routinely treat patients with postoperative antibiotics except for complex revision cases with multiple grafts, allografts, or previous history of infection. Local infiltration anesthesia of the entire external and internal nose is performed with lidocaine 1% with 1:100,000 epinephrine mixed in equal parts with bupivacaine 0.5% with 1:200,000 epinephrine. This provides long-acting anesthesia with a satisfactory vasoconstrictive effect. About 15 to 20 mL is required. We do not find added topical vasoconstriction to yield any additional benefit.
Surgical Technique
Incision Planning and Exposure
Some surgeons, primarily not in favor of the open technique, have cited the columellar scar as a major disadvantage of this procedure. However, if designed and closed judiciously, this is rarely a cause for revision. Large volume, retrospective studies by Foda of patients who underwent cosmetic open rhinoplasty revealed a subjective dissatisfaction incidence of less than 2%. 12 , 13 The first step in obtaining an ideal scar is incision planning. Our preferred open rhinoplasty incision involves a transverse inverted gull-wing approach in the midcolumella or slightly below ( Fig. 34.8 ).
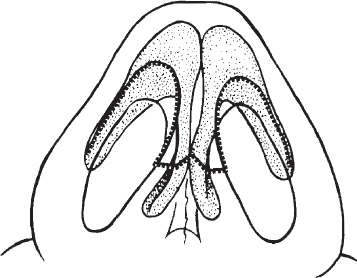
The gull-wing incision heals better aesthetically than V-shaped, staircase, or straight transverse incisions. It should curve around the caudal margin of the medial crus to meet the marginal incision at right angles. The marginal incision is placed just behind the caudal margin of the medial crus as this allows for both a wider columellar flap and improved scar camouflage. Care is taken to place the incision above the feet of the medial crura, especially in black and Asian patients in whom these structures are often foreshortened, and who are at risk for postoperative columellar notching. The columellar flap should be handled delicately to avoid jeopardizing its vascularity. The junction of the transverse columellar and vertical marginal incisions is most at risk for an unfavorable scar as forces of contraction tend to cause a trapdoor effect in this location. This effect can be minimized through undermining of the inferior columellar skin prior to closure, and by placement of the angle suture full thickness inferiorly but only partial thickness superiorly, to “tuck in” the thicker superior flap edge. A single, simple inverted 6-0 polyglycolic acid suture may be placed intradermally in the central columella to decrease tension. We prefer simple 6-0 nylon everting skin sutures alone for columellar closure. In cases where significant deprojection of the tip has been performed, the columellar flap may be slightly long. Truncation of the flap by 1 or 2 mm will diminish the risk of a mild hanging columella effect in this instance. Conversely, when significant tip projection has been achieved, the columellar flap may appear relatively short on closure. Closing tension can be relieved by bilateral inferior extension of the vertical marginal incisions, allowing development of an inferior columellar advancement flap. If this potential problem is recognized preoperatively, a V-shaped columellar incision may be later closed in a V-to-Y fashion to achieve a similar columellar lengthening, although this tends to leave a slightly inferior scar.
The transverse columellar incision is made initially with a no. 11 blade. It is joined with a vertical marginal incision made superficially, so as not to incise the underlying crus, beginning at the soft tissue triangle. The columellar flap is freed up with scissors dissection up to the angle. We prefer to carry blunt and sharp scissors dissection superolaterally over the dome and along the lower lateral crus, allowing exposure of the tip cartilages under direct vision. However, it is occasionally necessary to first make the marginal incision with retrograde exposure in cases of severe scarring or unusual lobular configurations that render scissors dissection over the domes precarious. Elevation of dorsal skin may be performed blindly as in the closed technique. In cases of severe scarring, poorly defined deformities, or thin skin, exposure is performed under direct vision with scissors or knife dissection. Bleeding from the inferior columellar artery or from branches of the facial artery in the region of the pyriform aperture may be controlled with conservative bipolar cautery. The dorsal skin is elevated in a submucoperichondrial and submucoperiosteal plane to diminish bleeding and tissue trauma. A balance is struck between maintenance of soft tissue support and skin elevation sufficient to allow appropriate surgical maneuvers and postoperative skin redraping.
Septal Deformities
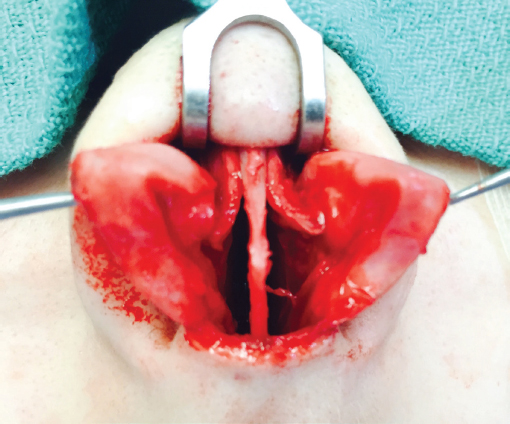
Septoplasty is usually performed first to correct functional problems and to obtain any cartilage that may be necessary for grafting. The superior septal angle is easily identified, and soft tissue is removed from between the medial crura down to the premaxilla. This provides excellent exposure of the caudal septum and allows the columella to be narrowed. This is especially helpful if a columellar strut is to be placed because struts widen the columella inferiorly. If nasolabial augmentation is required, this soft tissue may be retained as a flap based inferiorly and turned on itself to provide additional nasolabial angle augmentation. 14 It is secured with a throughandthrough premaxillary transfixion suture. More frequently, the soft tissue is excised to be used later as a camouflage graft if required. We often deepen or flatten the premaxilla at this juncture with a rongeur. The wide exposure offered by the open approach is much superior to closed techniques for this purpose. The nasal spine may be flattened to create an optimal platform for a columellar strut, but its excision is highly inadvisable. Beginning at the anterior septal angle, complete submucoperichondrial and submucoperiosteal septal flaps are elevated bilaterally. The upper lateral cartilages are separated from the septum such that the nasal dorsum and septum are ouvert au ciel, or open to the sky. This affords a superb undistorted view unavailable with closed techniques, allowing any desired septoplasty technique to be executed ( Fig. 34.9 ). Of note, the view is more anterosuperior than that seen in closed techniques and may require some adjustment of orientation in the mind’s eye.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


