61 Clinical Applications of Plating Systems to Facial Fractures
Introduction
Whether repairing fractures, fixing osteotomies, or reconstructing skeletal defects, the goal of the surgeon is to effect a bony union as rapidly and dependably as possible with limited morbidity and complication rates. Recent experience indicates that rigid skeletal fixation, when properly applied, is most likely to achieve these goals. There are numerous plating systems in use today, each with its own unique designs, instruments, plates, screws, and metals. Yet all systems have in common the following central principle: a screw screwed into a bone can remain tight and withstand functional stress over time. With this demonstrated, the following three principles support the various methods of rigid fixation in use throughout the craniofacial skeleton: (1) overlapping bone fragments can be screwed together stably with lag screws, (2) stability of fixation can be increased when fragments are compressed together with compression plates (though this technique is rarely applied to the maxillofacial skeleton today), and (3) plates screwed to bone fragments maintain and replace the structural integrity of damaged bone, even across a significant gap (bony defect). These principles form the foundation for the successful use of any bone plating system.
Initial attempts at plate fixation failed because of a lack of understanding of the biomechanical principles involved in bone repair. The earliest attempts at rigid fixation in facial bones were in mandible fractures, where improper plate positioning resulting from a lack of understanding of the tension and compressive forces acting on the mandible in function resulted in instability and, frequently, infection and failure. These failures were misunderstood and were thought to be due to excessive stability failing to provide the motion needed to effect bone healing. This misconception was corrected by research in orthopedic surgery. It was found that failures were due to inadequate (rather than excessive) stabilization. With a better understanding of the dynamic forces acting on bones, more stable fixations and high success rates were achieved. It was then some years before the biomechanical principles upon which proper stabilization of mandible fractures depends were elucidated. In the last three decades, facial plating techniques have gained wide acceptance as the advantages of rapid and effective healing with early function have become commonplace.
Bone Healing
Although osseous healing has been addressed in another chapter, a few comments are appropriate here. Bone healing depends on the stabilization of fractured or osteotomized fragments. Whether guided by medical intervention (e.g., cast, splint, fixation device) or allowed to occur spontaneously, bone healing generally ensues. Healing depends on the growth of osteons across the fracture or defect so that the injury is bridged by new bone. This new bone remodels in response to physiologic stresses, and healing is complete. However, motion disrupts the growing osteons. The body therefore produces a callus that stabilizes the fragments, allowing osteon growth and healing to proceed. The callus is nature’s rigid fixation device. Casting and splinting (e.g., mandibulomaxillary fixation [MMF]) and even interosseous wiring and external fixation partially immobilize the fracture and guide the position that the fragments will be in when the callus stabilizes them. If the degree of motion is too great or if infection intervenes, stabilization may not occur at all, and the gap may widen and fill with fibrous tissue. If this occurs, a nonunion (fibrous union, pseudarthrosis) frequently results. A pseudarthrosis, as its name implies, is essentially a fibrous union, and motion occurs where the bone fragments are held together by fibrous tissue, thus creating a “false joint” or pseudarthrosis.
When bone injury occurs, bleeding results in a fracture hematoma. Early ingrowth of blood vessels and fibroblasts begins the differentiation cascade of bone healing. The development of chondroblasts, the conversion of fibrous tissue to fibrocartilage, and ultimately the ingrowth of osteoblasts that lay down osteoid result in callus formation. 1 This process begins subperiosteally on either side of the fracture, and the callus grows across from both sides, bridging and stabilizing the fracture. The same process is repeated across the fracture site. Finally, osteons grow across this area, and remodeling completes the healing process. This natural process, like surgically assisted healing, is dependent on the ability of the callus to stabilize the fragments, which in turn allows for the ultimate bridging of the fracture by bone. If the forces acting on the fragments are so great that stabilization cannot occur, ultimate bony union will be unlikely. Furthermore, in the absence of surgical guidance, even if healing does take place, it will often be in a poor anatomical alignment (malunion). (Note that although remodeling in response to stress can result in normal bone strength, it will not correct a malocclusion, a problem unique to malunions [malpositions] of mandibular and maxillary fractures.)
Rigid fixation techniques are designed to stabilize the fractured fragments, thereby increasing the likelihood that bony union will take place (in the correct position) and minimizing the chance for nonunion. As mobility leads to callus formation, the greater the stability of the surgical fixation, the less callus that develops. Though microscopically there is always some callus formation, when a very rigid fixation is accomplished there will not be enough callus to show on X-ray. Therefore, the finding of a callus at the fracture site on radiographic evaluation of a patient after surgical repair has been used as an indication of inadequate stabilization of the fragments.
Application of Rigid Fixation Techniques to Mandibular Fractures
Occlusion
In any discussion of facial bone repair, a discussion of occlusion must take a central role. Regardless of the stabilization techniques used, the surgeon must reestablish occlusal relationships between mandibular and maxillary dentition before repairing fractures of the related bones. Whether arch bars or other MMF devices are required has become a controversial subject recently. However, by one means or another, MMF is generally applied before fracture repair, and the occlusion is periodically assessed to make certain that a malocclusion has not been created by osseous repositioning and repair. When a malocclusion is detected, the bones should be repositioned because a rigidly fixed malocclusion will not be improved by healing and bony remodeling. Proper occlusion is necessary for function; therefore, establishing a proper and functional occlusal relationship should be the priority in all but the severest of traumas. This generally means that if the appropriate position cannot be defined, use of a less rigid fixation (e.g., MMF alone) should be considered. When severe disruption of bone makes healing unlikely without rigid fixation, then the need to achieve healing and prevent infection may sometimes take priority over establishing the exact occlusion. This difficult and controversial clinical decision must be made by the facial plastic surgeon at the time of repair. Note that screws can be used for establishing occlusion, and new types of arch bars can even be screwed in place, though it is important to recognize that these techniques can pose risks to tooth roots. Two screws can be placed in the maxilla and two in the mandible, and wires can be tightened around these, thereby establishing MMF. Specially designed screws with large, protruding heads and holes through which the wires can be passed have been produced specifically for this purpose. Note that although this method is fast and simple, it is not an ideal technique because tightening of the wires tends to create lingual version of unstable fragments due to the buccal positioning of the fixation points. The screw-in arch bars are designed to overcome this problem and provide more fixation points for MMF.
Biomechanics
Proper use of rigid fixation requires placement of fixation devices so that immobilization of the fracture fragments is accomplished during motion as well as when the bones are at rest. The forces acting on the mandible are complex and variable, shifting depending on the site of the food bolus being chewed and the status of the dentition. To effectively stabilize the fragments, the surgeon must have some understanding of the forces of distraction that will be generated by muscle activity so that these can be overcome. Failure to accomplish this adequately can lead to motion around the implant during function. Not only does this increase the likelihood of implant failure and nonunion, it also increases the probability of wound infection and, ultimately, osteomyelitis. (The surgeon, believing that the plate has created stability, may be unaware that adequate fixation was never accomplished, and rigid fixation will be blamed for the failure.) Proper understanding of the biomechanics of the mandible in function will lead the surgeon to apply the appropriate number of plates of the correct size and strength in the proper position. When the forces of distraction are overcome by the fixation appliance, healing occurs most dependably and frequently, and the failure rate is kept to a minimum. Therefore, it is necessary to be familiar with the functional forces operating on the mandible in each anatomical area, and plate fixation techniques must be applied in each area to overcome the distracting forces and to take advantage of the naturally occurring compressive forces.
Most bones do not bear weight symmetrically, so that in function there are generally areas that are under pressure and areas that are under tension. Fig. 61.1 is an extremely oversimplified depiction of the forces affecting the mandible during chewing. In Fig. 61.1a , the plus signs indicate the compressive forces acting on the mandible during mastication and the minus signs show areas under tension. When a fracture occurs, these forces tend to distract the tension side of the fracture, whereas the fragments will be compressed together at the pressure side ( Fig. 61.1b ). Although this represents a markedly oversimplified description of the forces acting on the functioning mandible, the concept of tension and compression areas is fundamental to the proper placement of miniplates and compression plates for the repair of mandible fractures. This important biomechanical concept was first appreciated in the study of long bone fracture repair. 2 Initially, it was thought that a rigid plate fixed to two pieces of bone with two fixation points in each fragment would create a stable fixation and prevent movement of the fragments relative to the plate and to each other. Early clinical failure in both the long bones and the mandible can be attributed to this misconception. Thoughtful analysis reveals that a rigid plate with two fixation points in each of two fragments can provide stability only if the forces transmitted to the plate and screws in functional loading are less than the strength of the plate and the forces holding the screws in place. When plates and screws of proper design and tensile strength are correctly positioned and applied according to biomechanical principles, stability is achieved and healing usually results. In fact, adequate plate and screw design was achieved early; proper plate positioning was understood later, when tension and compression forces were appreciated.

Using the femur as an example ( Fig. 61.2 ), it should be intuitively apparent that weight bearing on the femoral head produces distracting forces on the lateral cortex and compresses the medial cortex. A plate placed on either cortex (across a fracture) holds the fragments together at rest, and a compression plate adds a positive (compressive) force across the fracture. In function, however, the distracting forces on the lateral cortex generally exceed the compressive forces of a medially placed plate; therefore, the dynamic forces vary from positive (rest) to negative (weight bearing). Screw loosening frequently results, and motion leads to nonunion and even osteomyelitis. On the other hand, when the plate holds the tension side together, distraction cannot occur unless a screw fails, and the compressive forces of weight bearing are added to any static compressive forces applied by the plate and distributed across the fracture. Although the forces across the fracture vary, they never become negative (distracting), and healing generally ensues.
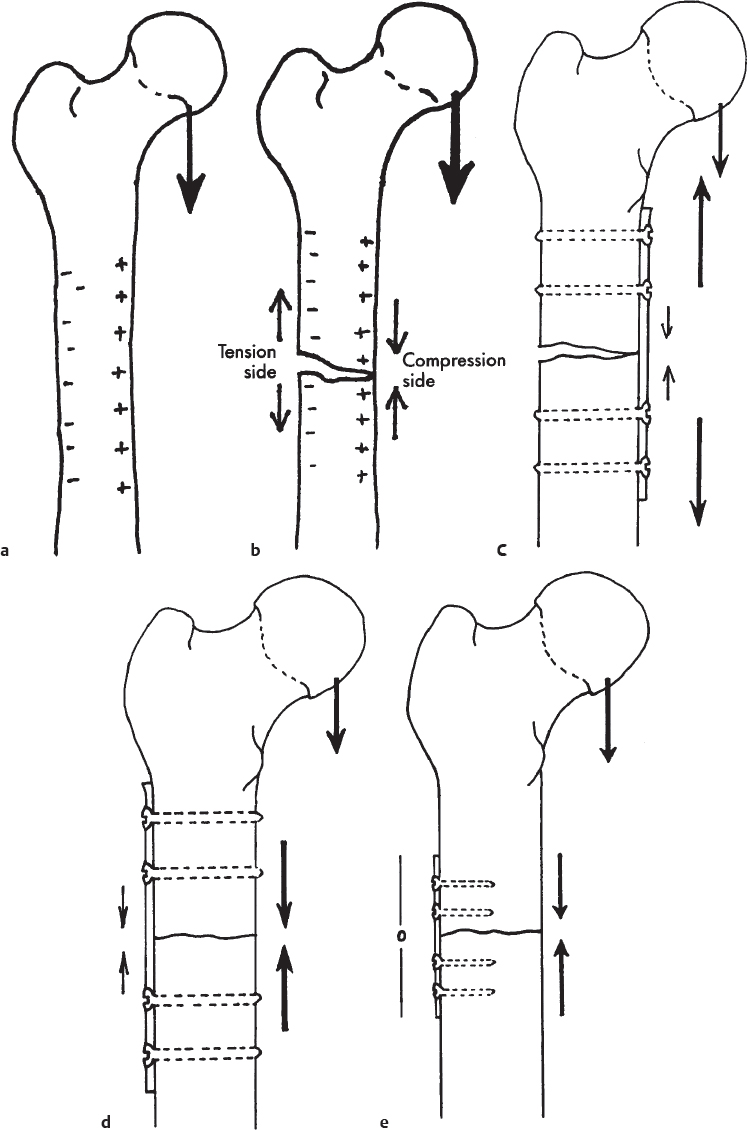
It should also be apparent that the more biomechanically advantaged the repair, the less dependent it will be on the size and strength of the hardware. When repairing a fracture in an area of tension, as long as there is extensive bony contact in the compressive area and minimal torque on the fixation point, small fixation appliances (as long as they can overcome the distracting forces at the site of placement) will generally prove adequate. On the other hand, when large distracting and rotational forces are found in areas with weak bone or minimal contact areas between the fragments (as in the atrophic mandible), larger fixation devices will generally be necessary. The most extreme example is an area of bone loss, in which case the implant used (if no bone replacement is performed at the time of repair) must be large and fixed with large screws using multiple fixation points.
Armed with an understanding of the above principles, the reader should see why certain techniques of mandibular repair succeed and why others fail.
Arch Bar Fixation with Mandibulomaxillary Fixation
It has long been thought that MMF splints the mandible in a fixed position and puts it at rest. This is not entirely true, and even swallowing generates large forces across the mandible. However, since a well-placed mandibular arch bar puts tension across the teeth, it holds the area of distraction together. If there is large bony contact, and the torsional forces are minimal, the mandibular arch bar creates enough stability to allow a callus to form, and healing results. Of course, the significant failure rate seen when MMF alone is utilized has led to a need for more dependable fixation techniques (along with a desire to avoid prolonged periods of MMF).
Mandibulomaxillary Fixation with Interosseous Wire Fixation
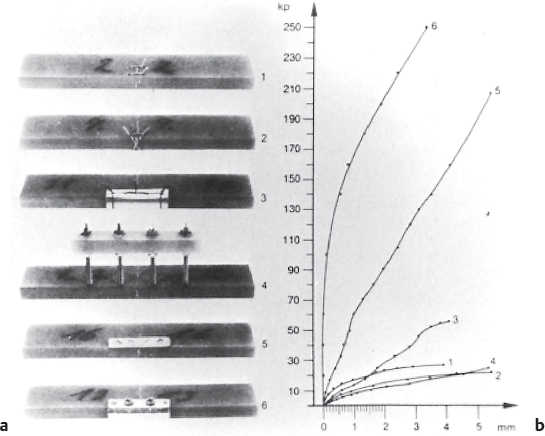
Interosseous wire fixation was added to MMF in an effort to overcome the high failure rates seen when MMF was used for unstable fractures. When the wire repair was placed in the biomechanically advantaged tension areas of the mandible, success rates improved. However, when failures occurred, the presence of the wire frequently resulted in a foreign body infection and osteomyelitis was common. Prolonged periods of MMF were also required and when delayed union occurred, MMF could be needed for as long as 6 to 12 months. Furthermore, although many surgeons believed that complex, basketweave types of wire placement provided marked stability, the early work of Luhr 3 demonstrated the weakness of wire fixation—and even external fixation—compared with fixation with plates and screws ( Fig. 61.3 ).
Miniplate Osteosynthesis
This is the historical name applied to the plating techniques most commonly utilized today for repair of craniomaxillofacial fractures. It is contrasted with compression fixation (rarely used) and reconstruction plate fixation, both of which require the use of larger plates and screws. In an effort to improve techniques of mandibular fracture repair, Champy studied the biomechanics of mandibular fractures and found that a properly positioned miniplate can often take advantage of the dynamic compressive forces occurring in function. 4 A miniplate placed along the tension side of a fracture holds it together at rest without compression; under functional loading, when the fixation is strong enough to hold (i.e., to merely withstand the distracting forces), compression of the fracture fragments results ( Fig. 61.2e ).
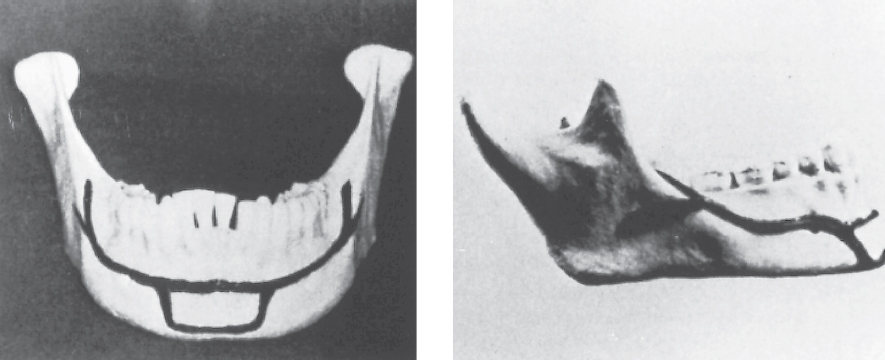
The success of this approach for the repair of mandibular fractures depends on several factors. First, it is critical to determine where the miniplates must be applied to effect the stabilization necessary for healing. This was painstakingly accomplished by studying the lines of force generated by various miniplate fixation points, using araldite models to simulate mandible fractures. Using this approach, Champy was able to define the areas for miniplate fixation along the so-called ideal osteosynthesis line 5 ( Fig. 61.4 ). This line corresponds to the line of tension along the mandibular body. From parasymphysis to parasymphysis, two miniplates are required to overcome the torsional forces affecting this area. Posteriorly, a single miniplate along the oblique line or below it was thought to be effective; however, Kroon 6 has shown that the forces in this area vary from positive to negative during function, necessitating the use of a second plate inferior to the first if dependable stabilization and healing are to be achieved. Whether to use one or two miniplates when repairing a fracture at the mandibular angle remains controversial. Levy et al 7 have shown that the complication rate when repairing mandibular angle fractures with miniplates drops from 26% when a single plate is utilized to 3% when a second plate is added. This is consistent with the findings of Kroon. 6 Ellis and Walker, 8 on the other hand, found a single plate not only to be adequate but to yield better results. However, they encountered a 16% complication rate in this group (compared to 28% when they used two miniplates), which is not as good as the 3% rate of Levy et al, when two miniplates were used. Until this controversy is resolved, the author recommends the use of two plates if a miniplate technique is utilized to repair a fracture of the mandibular angle region.
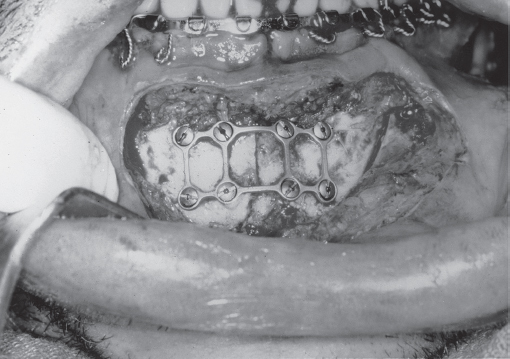
With the ideal plate position identified, the osteosynthesis line overlying the inferior alveolar nerve and tooth roots remains a problem. The solution is the monocortical screw. A monocortical screw penetrates only the lateral cortex of the mandible, and great care is exercised to avoid deeper penetration into the alveolar nerve and tooth roots. When performing these procedures, the surgeon must be aware of the location of the tooth roots and of the inferior alveolar nerves. It should also be clear that the use of monocortical screws precludes the application of compression because compression plating puts pressure on the screw shaft at its entry point into the bone; the thin monocortical fixation of the screw to the bone will likely be inadequate to prevent shifting of the screw, which would lead to loosening and failure. Nonetheless, the plates and screws used must be strong enough to resist the distracting forces that occur in function. Two-millimeter mandibular miniplates are designed to overcome these forces, and, when properly applied, fixation failure is uncommon. However, many failures have resulted from the use of inadequate fixation, as may be seen when weaker plates designed for midfacial applications are applied to the mandible. The facial plastic surgeon must be familiar with the systems and must be sure to select implants designed for the particular indications for which they are being used. Similarly, the screws must be of appropriate size, strength, and number, and they must hold tightly in the bone. If a screw hole strips during screw tightening, it must be abandoned, as it will not provide fixation. A larger (“emergency”) screw may be utilized or the plate must be moved and new holes used. A variation of the miniplate technique is the use of the “threedimensional plate” applied along the line of tension as described by Farmand. 9 The threedimensional plate is actually a miniplate that has been strengthened by being produced in geometric assemblies of squares and rectangles ( Fig. 61.5 ). Although the plates are slightly more difficult to bend, the results using them have been excellent.
Compression Osteosynthesis
This technique is rarely applied to maxillofacial fractures. However, familiarity with the principles is still of value. As the name implies, compression osteosynthesis involves the application of a force across the fracture such that the fractured fragments are compressed together by the fixation. Thus, at the time of fixation there is a compressive force between the fragments at rest. This is in contrast to miniplate fixation, in which case the bone fragments are held together without compression, so that compressive forces are only seen across the fracture during function (if the plate has been properly positioned and applied). Whereas it was originally believed by the proponents of compression plating that the compressive forces were necessary for direct bone healing, it is now clear that healing takes place quite dependably when neutral fixation is properly applied. However, compression certainly increases the area of bone-to-bone contact as well as the frictional forces between the fragments, so that the likelihood of successful healing, particularly in a complex and unstable fracture, is probably increased. Compression fixation may also be accomplished with lag screws, as will be described below. Note that when compression is applied across a fracture, the bone remodels under the stress to eliminate the force until the plate and/or screws are ultimately exerting no force on the bone. However, this remodeling is occurring during healing, so that a complete bony union has resulted by the time the force exerted by the fixation appliance has dissipated.
Compression Using a Plate
The technique for compression using a plate is described at the end of this chapter. As noted above, compression plate stability requires the use of bicortical screws (to prevent motion of the screws in the bone and failure of the fixation). Since the presence of the tooth roots and the inferior alveolar nerve prevents the placement of bicortical screws in the biomechanically correct position along the line of tension, compression plates are placed along the basal border of the mandible (below the inferior alveolar nerve). Despite the use of strong plates and large screws, this biomechanically incorrect positioning is frequently inadequate to overcome the distracting forces that develop across the fracture during function ( Fig. 61.6 ), and, in fact, early experiences using this technique resulted in unacceptably high failure rates and frequent condemnation of the technique.
However, this problem was overcome by Spiessl with the use of tension banding. 2 , 10 A tension band is applied to hold the traction side of a fracture together. This is analogous to the miniplate applied along the ideal osteosynthesis line. Compression can then be applied to the pressure side without distracting the traction side. Furthermore, the compressive force applied will be distributed along the full length of the fracture. This compressive force increases the friction and contact between the fragments, thereby increasing the rigidity of fixation and the likelihood that bone healing will occur.
A tension band can be applied in several ways. When a fracture occurs in a dentulous area of the mandible, an arch bar attached to the teeth across the fracture line can serve as a tension band. This must be tightly applied so that distraction does not occur along the alveolar segment when compression is applied at the basal border. Behind the dentition, a plate can be placed above the level of the inferior alveolar nerve to serve as a tension band, and a compression plate can then be placed at the basal border. This is similar to the miniplate approach, and, in fact, a miniplate can also serve as a tension band for use in conjunction with a basally positioned compression plate for any mandibular fracture.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


