6 Gluteal Artery Perforator Flap for Breast Reconstruction
Richard Mahlon Kline, Jr., and James Ernest Craigie
In 1994, Robert J. Allen presented the gluteal artery perforator (GAP) flap for breast reconstruction at a meeting of the American Association of Plastic Surgeons in St. Louis, Missouri. Since that time, GAP flaps have become a reliable option for muscle-sparing autogenous tissue breast reconstruction. Advancements in the field of perforator flaps have increased the donor sites available to microsurgeons for breast reconstruction. Breast reconstruction scenarios are as varied as the human body in regard to shape, form, and volume requirements. When the perforator concept is employed, skin and fat are harvested without requiring removal of the underlying muscle. Also, emphasis is directed away from larger named blood vessels, donor sites confined to a template over certain muscles, and familiar anatomic landmarks. This enables a patient’s donor site to be designed based on their distribution of fat and body shape. GAP flaps have been used when the lower abdominal tissues are inadequate to meet the desired result or when previous surgery compromised the lower abdominal perforators. When both the abdomen and the buttock are available and both meet the volume requirement, the flap of choice can be based on the patients’ preference about donor-scar location. This is particularly the case in patients who are thinner and who would not benefit from a tummy tuck.
Indications
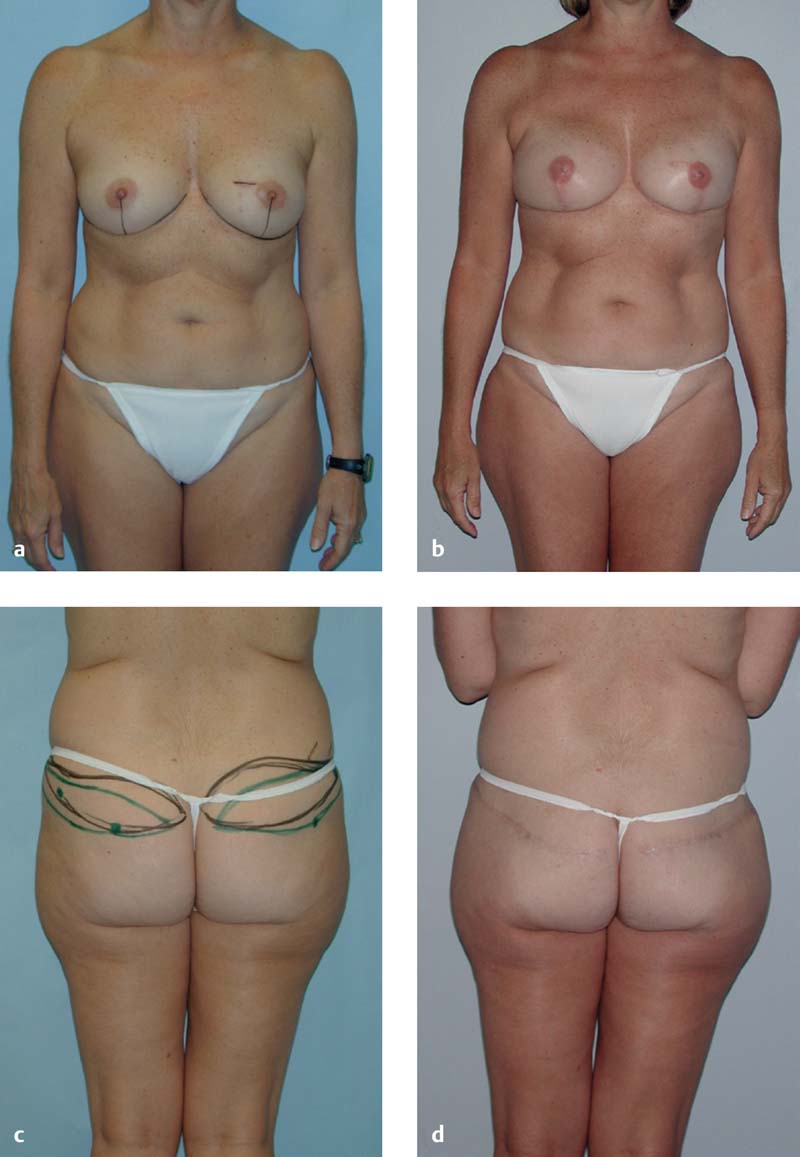
Gluteal artery perforator flaps are used for unilateral and bilateral cases. Breast reconstruction indications include developmental aplasia and postmastectomy cases. GAP flaps are utilized following mastectomies for both cancer and prophylactic indications. Immediate reconstruction cases include nipple-sparing and skin-sparing mastectomies ( Fig. 6.1 ). When radiation is indicated, a delayed reconstruction may be required following recovery from the radiation. Delayed reconstructions include failed implant cases and failed previous free flap procedures. A superior gluteal artery perforator (SGAP) flap can provide reasonable symmetry with a contralateral breast previously reconstructed with a deep inferior epigastric perforator (DIEP) flap. The gluteal fat and skin can be a very close match for a contralateral DIEP.
Preoperative Planning
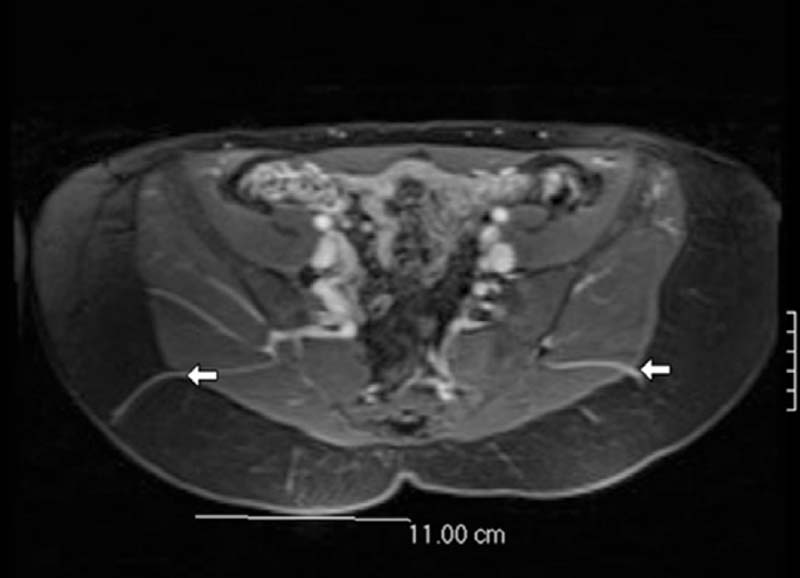
Two microsurgeons who are experienced with perforator techniques and principles work together on each case. The primary surgeon meets with the patient the day before surgery at the presurgery planning appointment. At this time surgical markings are placed based on a review of the magnetic resonance angiogram (MRA) and the use of the handheld Doppler. Preoperative imaging with an MRA or a computed tomography angiogram (CTA) greatly enhances the application of the gluteal donor site and the perforator flap concept. Imaging combined with a handheld Doppler exam enables more detailed tailoring of the flap and is particularly helpful for bilateral simultaneous GAP (BSG) flap harvesting.
During the presurgery marking, the MRA is reviewed in detail.1 The location of the largest GAPs are described by the radiologist using a coordinate system. Each large perforator is measured from a midline reference point on the patient’s skin. The reference point is the top of the gluteal crease or tip of the coccyx. The radiologist records the horizontal distance and the vertical distance from the reference point. The perforator location is measured at the point it leaves the muscle, and the location is extrapolated to the position on the skin where the Doppler signal will be heard. It is important to note that the both the MRA and markings are performed with the patient in the prone position.
The images are reviewed, and the best perforators are chosen with regard to size, location, distribution of fat around the perforator, and the intramuscular/submuscular course of each vessel. For a bilateral case, note is made of the most symmetrical pair of perforators on the right and left side ( Fig. 6.2 ). There are two important points to note: (1) whether a perforator is located in the medial or lateral third of the flap, and (2) whether there is a septocutaneous (sc) GAP between the gluteus maximus and medius muscles.2 The more lateral perforators and sc-GAP will have a more tangential course around the gluteus maximus muscle and result in a longer pedicle, which is preferred. The medial perforators will have a more direct intramuscular course and shorter pedicle. Perforator selection is important for symmetry and for exposure during the microsurgical anastomosis.
If the MRA reveals large laterally positioned perforators, then the flap can be designed more laterally away from the gluteal crease and centered over the thicker fat and large perforator. Also, this places the resulting scar in a more aesthetic position, as it can be covered by underwear or a bathing suit.
The mastectomy defect is measured first or anticipated for immediate reconstruction so that the flap dimensions can be adequate. Caution is needed in patients with large skin requirements, particularly radiation defects. GAP flaps have a lower skin-to-fat thickness ratio and lower skin coverage compared with abdominal skin flaps. Typical skin paddle dimensions are 8 to 9 cm vertically, but occasionally 10 to 11 cm may be needed for significant skin deficits. If it is more than 12 cm, it may be difficult to close, and skin laxity of the donor site should be considered. The width of the skin paddle design varies more with the patient’s shape but is typically 20 to 24 cm. Beveling is used to maximize the volume of harvested fat, so that upon reaching the muscle, the flap is longer and wider than the skin measurements. The base measurements are typically 12 to 14 cm, compared with an 8- to 9-cm skin pattern.
To aesthetically design the flap, the patient is marked first in the standing position so that the first flap design is over the most favorable contour of the buttock region. These marks are made without specific reference to the MRA measurements. Care must be taken to make sure the flap is not positioned too high. To avoid missing the dominate perforator, the patient is next marked in the prone position. A second pattern is designed at this time with specific note of the MRA measurements.
The markings are photographed with the patient in the standing position. The photo is taken to the operating room along with the MRA report measurements and the actual MRA disk for use during the surgery. The final markings include skin pattern and fat beveling outlines ( Fig. 6.3 ). This becomes very important during bilateral simultaneous flap cases. The primary surgeon performs the markings, but both microsurgeons elevate a flap simultaneously, and the end result must be symmetric. It may be helpful to estimate flap weight at the beginning of the procedure and to attempt to shape the flap accordingly. Results improve with experience and with the surgeons working together.

Related posts:
 2 Starting a Perforator Flap Breast Program
2 Starting a Perforator Flap Breast Program
 10 Bipedicled (Double or Stacked) Abdominal Perforator Flap in Unilateral Breast Reconstruction
10 Bipedicled (Double or Stacked) Abdominal Perforator Flap in Unilateral Breast Reconstruction
 9 Pedicled Lateral Thoracic Flap for Breast Reconstruction
9 Pedicled Lateral Thoracic Flap for Breast Reconstruction
 13 Lateral Thigh Perforator Flap (Septocutaneous Tensor Fasciae Latae Perforator Flap)
13 Lateral Thigh Perforator Flap (Septocutaneous Tensor Fasciae Latae Perforator Flap)
 15 Deep Circumflex Iliac Artery Perforator Flap for Breast Reconstruction
15 Deep Circumflex Iliac Artery Perforator Flap for Breast Reconstruction
 11 Venous Salvage Procedures in the Deep Inferior Epigastric Perforator Flap for Breast Reconstruction
11 Venous Salvage Procedures in the Deep Inferior Epigastric Perforator Flap for Breast Reconstruction
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


