55 Thumb Basal Joint Arthroplasty: Trapeziectomy
Abstract
Trapeziectomy has emerged as the most likely standard-of-care procedure for recalcitrant symptomatic thumb carpometacarpal arthritis. Whether performed alone or with adjunct techniques, knowing how, and being able, to successfully accomplish this procedure is a critical basic skill for all hand surgeons to master. In this chapter, we describe our preferred method for trapeziectomy along with relevant important considerations and lessons learned relative to the technique.
55.1 Description
There are a variety of distinct surgical procedures that have been described for treating various stages of thumb basilar, or carpometacarpal (CMC), joint arthritis. These procedures include but are not limited to trapeziometacarpal capsuloligamentous reconstruction, metacarpal osteotomy, CMC arthrodesis, joint replacement, denervation, and partial or complete trapeziectomy. Trapeziectomy can be performed independently or augmented with other procedures, with the most common ones being tendon interposition (TI), ligament reconstruction (LR), or ligament reconstruction combined with tendon interposition (LRTI). In this chapter, we focus on simple trapeziectomy.
55.2 Key Principles
The primary pain generator in basilar thumb degeneration is thought to be the CMC joint, involving the base of the thumb metacarpal, trapezium, and supporting capsuloligamentous and nerve structures. In addition to addressing the thumb CMC arthritis, it is important to assess and address other potential pain and disability generators in the region, such as scaphotrapezoidal degeneration, distal flexor carpi radialis (FCR) tendinosis, thumb metacarpophalangeal (MCP) hyperextension or degeneration, first extensor compartment tenosynovitis (de-Quervain’s disease), and carpal tunnel syndrome.
55.3 Expectations
Trapeziectomy alone has comparable outcomes to trapeziectomy with LRTI or other thumb CMC arthritis procedures, is more cost effective, is less technically demanding requiring less operative time on average, and in some studies has fewer complications such as reoperation, complex regional pain syndrome, and infection.
55.4 Indications
Symptomatic, radiographic-proven osteoarthritis of the thumb CMC joint which has failed nonoperative measures.
55.5 Relative Contraindications
Eaton stage I (inflammatory stage without degenerative changes on X-ray) osteoarthritis.
Recent thumb CMC intra-articular corticosteroid injection: in keeping with other orthopedic surgery evidence and recommendations, we typically recommend waiting 3 months after an injection before proceeding with surgery, although we are not aware of any studies which have corroborated this for trapeziectomy specifically.
55.6 Special Considerations
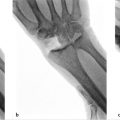
We recommend routine preoperative radiographic assessment of the patient’s anatomy, which helps with identifying osteophytes, loose bodies, and any other joints in the area with degenerative changes. However, advanced imaging is not required or recommended for standard preoperative planning.
55.7 Special Instructions, Positioning, and Anesthesia
Place patient supine on operating table and the upper extremity on an operating arm board.
Apply pneumatic tourniquet for adequate visualization and hemostasis; using local anesthetics with epinephrine and no tourniquet or regional anesthesia is an option to diminish or eliminate the need for sedation or general anesthesia as well.
55.8 Tips, Pearls, and Lessons Learned
Remove trapezium in one piece if possible. We have found that removing the trapezium as a whole saves operative time. We also evaluate with inspection and palpation of the entire area, after trapeziectomy, to identify any residual loose bodies or metacarpal base osteophytes.
Assess scaphotrapeziotrapezoidal (STT) joint preoperatively, and the scaphotrapezoidal joint after trapeziectomy, to determine if this could be another pain source in the area. Intraoperative assessment of the articulation between the trapezoid and distal scaphoid directs decision-making as to whether to proceed with partial or complete trapezoidectomy or limited fusions as required. Unlocking a degenerative STT joint may inadvertently lead to the development or worsening of radiographic dorsal intercalated segment instability of the carpus, although this may not correlate with a development or increase in symptoms.
Evaluate the distal FCR tendon in the base of the joint after trapeziectomy and debride or excise if you visualize significant degeneration. We think this could also be a postoperative residual pain source similar to the long head biceps tendon in the shoulder joint, which is often tenotomized, although we are aware of no investigative studies to corroborate this as of yet.
55.9 Key Procedural Steps
Some surgeons like to use a sterile finger trap on the thumb with weights hung off of the end of the arm board to provide traction for the procedure, but we do not routinely do so. Our preferred skin incision is dorsal, curvilinear, and centered over the trapezium. We place two incision-marking dots with one at the tip of the radial styloid and one just distal to the thumb CMC joint at the central dorsal base of the metacarpal. The incision is then drawn in an S-shape between these dots, curving from proximal palmar to distal dorsal (► Fig. 55.1). After the skin incision is made, any superficial branches of the radial nerve and lateral antebrachial cutaneous nerve are protected, and the interval between the extensor pollicis brevis and longus is opened longitudinally (► Fig. 55.2).
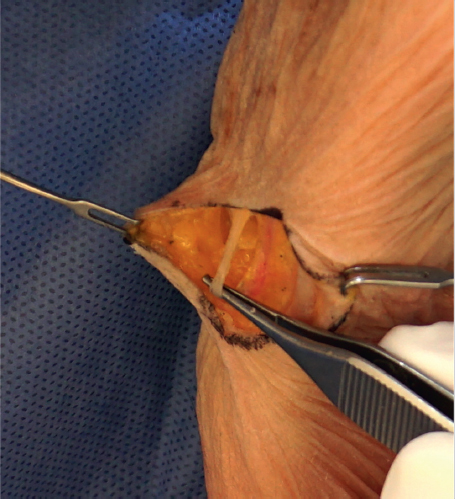
Next, we identify, mobilize, and protect the dorsal branch of the radial artery. The orientation of this vessel is variable, sometimes traveling longitudinally or transversely through the surgical field but most often at about a 45 degree angle off of the longitudinal axis of the thumb ray and in line with the central portion of the skin incision (► Fig. 55.3). We carefully mobilize the vessel proximally until it can be retracted proximal to the STT joint without undue tension. When mobilizing the vessel, we use bipolar cautery for the branches to the thumb CMC joint.
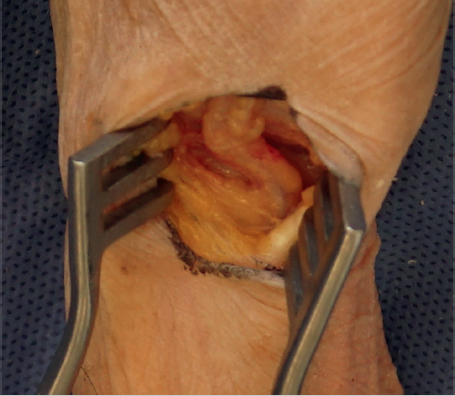
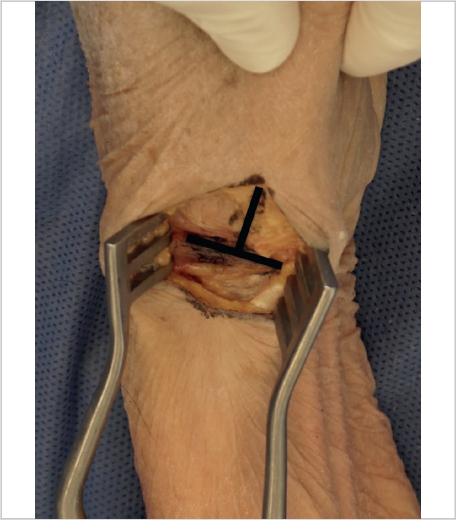
An inverted “T” capsulotomy is then performed with the longitudinal portion starting at the thumb metacarpal base distally, and extending over the trapezium proximally and the transverse portion at the STT joint (► Fig. 55.4). Capsular flaps are then elevated radially and ulnarly off the trapezium, being careful to maintain the capsular attachments at the thumb metacarpal base. We use a scalpel to release circumferentially about the trapezium to a depth of about half of the trapezium.
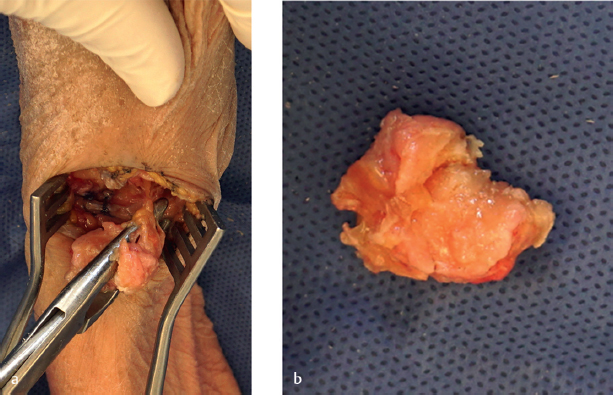
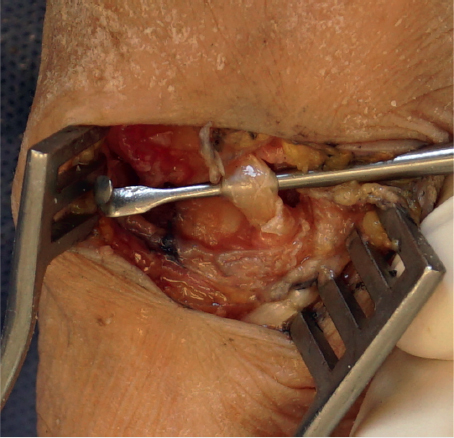
Next, we use a small, approximately one-fourth inch, osteotome to push away the capsule at the base of the trapezium circumferentially. We do not use a mallet for this; instead, we just use the osteotome as a dissecting tool. We push through this capsular base carefully around the trapezium, so as to not damage the FCR, flexor pollicis longus, and median nerve below. When pushing through the deep capsule, a slight “pop” is felt or heard. If the trapezium is not freely mobile at this point, the osteotome can be used to elevate under the deep side of the trapezium as well. Once the trapezium can be toggled easily with forceps, it is typically ready to be removed in its entirety with a Rongeur. We prefer the Leur Rongeur for this, which is the Rongeur with short, stout, and slightly curved ends. It straddles the proximal-distal sides of the trapezium all the way to the crux of the jaws. Next, the trapezium is gripped with the Rongeur and gently rotated in one direction without pulling up on the trapezium. Once the trapezium can be turned several times, it is ready to be pulled out of the joint (► Fig. 55.5). If there were significant osteophytes/degeneration about the base of the trapezium, the FCR may show signs of significant degeneration as well, but otherwise the distal FCR should remain pristine with this technique (► Fig. 55.6).
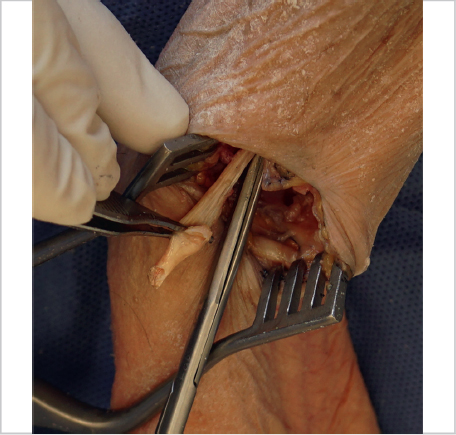
Next we inspect and palpate for loose bodies and capsular bone fragment remnants in the space, especially between the thumb and index metacarpal bases. We pull the FCR out of the wound with a Ragnell or similar retractor, with the wrist flexed in order to inspect as much of it as possible. If there is significant degeneration to the point where we think this could be a continued pain generator for the patient postoperatively, then we will transect it in the base of the wound as proximal as possible and allow it to retract proximally. We then dissect out the remaining FCR as distally as possible toward the index metacarpal insertion, transect, and remove it (► Fig. 55.7).
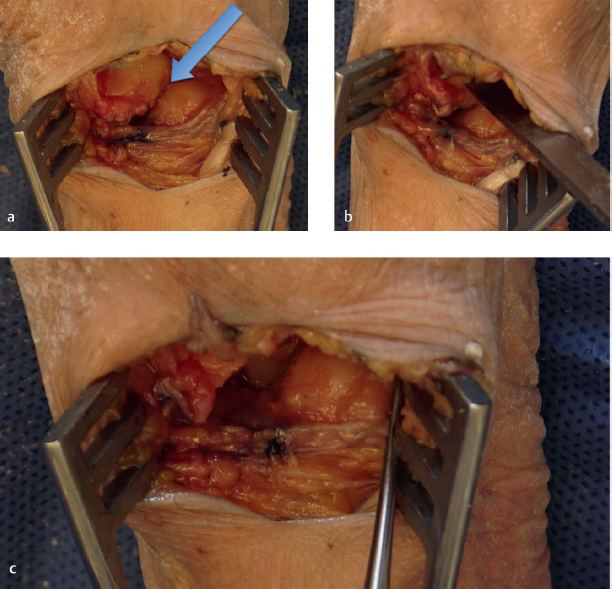
We then explore the scaphotrapezoid joint for any significant degeneration. This is best accomplished with manual traction of the index finger ray and gentle probing with a Freer elevator. If there is significant wear at the proximal trapezoid or distal scaphoid, we will use a sharp osteotome and mallet to remove however much of the proximal base of the trapezoid is involved. Once this is removed, we put the joint through a range of motion to insure there are no residual areas of potential pain generation or impingement. We continue this process until confirming no residual issues, and then load the index ray longitudinally to confirm no instability (► Fig. 55.8).
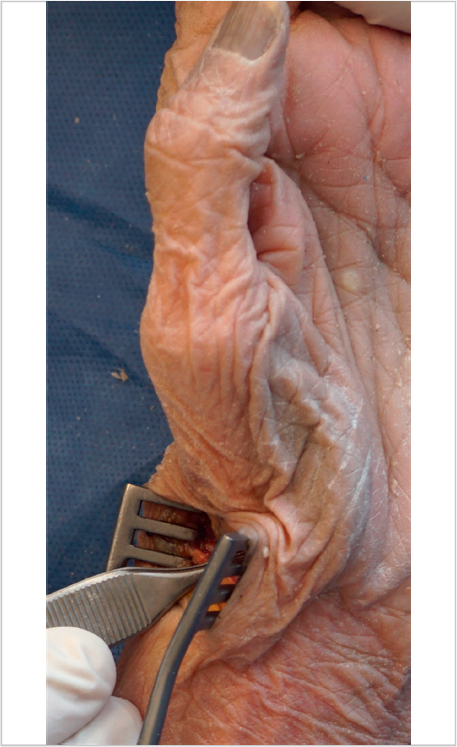
The wound and joints are copiously irrigated until clear. The previously made inverted “T” dorsal capsulotomy is closed longitudinally first, with absorbable figure-8 sutures, for which we favor 4–0 Monocryl. Then, the proximal transverse portion of the capsule is closed while holding the thumb metacarpal base in extension. After this capsular closure, the thumb should rest with the metacarpal base in slight extension (► Fig. 55.9). This counteracts its prior tendency for flexion and MCP hyperextension, the socalled Z-collapse deformity. If thumb MCP hyperextension needs to be addressed with volar capsulodesis or fusion, we perform that after trapeziectomy but before capsular closure. If a tourniquet was used, it is released at this point and hemostasis is obtained with special attention to the dorsal radial artery and its venae comitantes. We prefer 4–0 Monocryl subcutaneous buried interrupted sutures and adhesive strips for skin closure. A sterile dressing is applied, followed by a wrist thumb spica plaster splint, with the thumb metacarpal base in slight extension and the MCP joint in slight flexion.

Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


