56 Ligament Reconstruction Tendon Interposition (LRTI)
Abstract
Trapeziectomy and ligament reconstruction tendon interposition (LRTI) is an excellent form of treatment for thumb basal joint arthritis in the carefully selected patient. A complete trapeziectomy appears to be the critical portion of the procedure. Suspension of the metacarpal with flexor carpi radialis (FCR) is a commonly performed portion of the procedure, although it has not been demonstrated to improve outcomes. En block resection of the trapezium can be easily performed with the help of the techniques described. Reproducible and efficient complete trapeziectomy decreases operative time and likely results in less soft tissue trauma. Suspension of the base of the thumb metacarpal can similarly be performed simply with precision in order to create the bone tunnel and pass the FCR tendon. Pitfalls including tunnel fracture and transection of the FCR tendon can be mitigated by employing the techniques described.
56.1 Description
Gervis described trapeziectomy for the management of basal joint arthritis in 1949. While relieving pain in most cases, trapeziectomy alone allowed gradual subsidence of the thumb ray and some degree of ongoing pain and weakness. A number of options for basal joint arthroplasty of the thumb have been described with the hope of improving outcomes to include ligament reconstruction tendon interposition (LRTI) using flexor carpi radialis (FCR) (Burton and Pellegrini), suspensionplasty with abductor pollicis brevis (Thompson), hematoma distraction arthroplasty (Meals), and numerous variations using implants such as anchors, buttons, screws, and artificial joints. Of these procedures, LRTI is, by far, the most common.
56.2 Key Principles
Surgical options are largely based on a common theme of complete trapeziectomy with and without suspension of the thumb metacarpal.
56.3 Expectations
No benefit has been definitively demonstrated when comparing trapeziectomy alone to one of the more complex procedures including LRTI. Pain relief and patient satisfaction are generally good to excellent. Grip strength and pinch strength seem to improve, with grip strength improving more dramatically. 1 Proximal migration does occur with LRTI but less so than without suspension of the metacarpal. 2 No significant correlation has been found between maintenance of arthroplasty space and clinical outcomes. 3
56.4 Indications
Advanced radiographic disease that has failed conservative management. May consider fusion of the thumb carpopmetacarpal joint for young, active, and high-demand individuals. May consider arthroscopy, dorsal extension osteotomy, or Eaton–Littler ligament reconstruction for younger patients or those without significant amount of degenerative changes on X-ray.
56.5 Contraindications
Young age.
High-demand activities.
56.6 Special considerations
Metacarpophalangeal (MP) joint hyperextension must be evaluated concomitantly during the planning stages for treatment of thumb carpometacarpal (CMC) joint arthritis. During pinch, MP joint hypertension can direct the first metacarpal base into a subluxated position, potentially stressing any ligament reconstruction. Preoperative examination should pay particular attention to dynamic joint collapse during pinch rather than static laxity. Treatment can include percutaneous pinning of the MP joint in slight flexion + / – extensor pollicis brevis tendon transfer, volar capsulodesis/sesamoidesis, or MP joint fusion based on severity.
56.7 Special Instructions, Positioning, Anesthesia
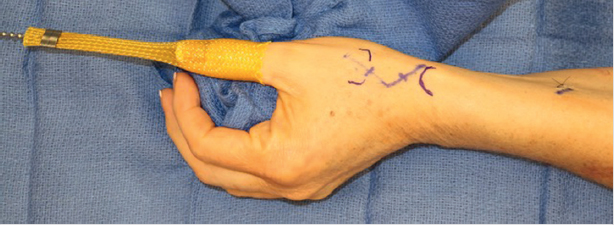
Supine, hand table, typically performed under general anesthesia or regional anesthesia with monitored anesthesia care and an upper arm tourniquet. Typically, fluoroscopy is not required. Traction with a finger trap and 5 to 7 lbs of weight hung off of the end of the hand table may be beneficial. This along with a small bump made from a single, rolled blue towel may provide good positioning without the use of an assistant for most patients (► Fig. 56.1).
56.8 Tips, Pearls, and Lessons Learned
56.8.1 Approach
Volar/Dorsal
The thumb basilar joint may be approached dorsally with an incision between the first and third extensor compartments or palmarly with an incision along the glabrous skin line. A dorsal approach is more widely used as the trapezium is directly subcutaneous and the incision avoids the palmar branch of the median nerve as well as the potentially irritable skin region of the wrist flexion crease. The dorsal approach requires meticulous attention to prevent injury to the superficial branches of the radial nerve.
The dorsal incision utilized by the authors is demonstrated in ► Fig. 56.2. Nerve branches should be maintained in the areolar tissue with the dorsal skin flap and not skeletonized or divided, which would risk neuroma formation and/or complex regional pain syndrome. The thin fascia between the first and third extensor compartments is incised longitudinally and a 2, 3 Weitlaner retractor placed.

Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


