5 Superficial Inferior Epigastric Artery Flap for Breast Reconstruction
Aldona J. Spiegel
Abdominal adipose tissue is the closest match in texture to breast tissue that the body has to offer. Because of this texture characteristic, abdominal tissue transfer has become the preferred choice in autologous breast reconstruction. To provide optimal care to breast reconstruction patients, techniques to minimize dissection of the abdominal musculature have been developed, which include the deep inferior epigastric perforator (DIEP) flap and the superficial inferior epigastric artery (SIEA) flap as methods of breast reconstruction.1 These flaps both involve the use of adipocutaneous tissue with the lower abdomen as a donor site ( Fig. 5.1 ).
In 1971, Antia and Buch2 published the first article on the SIEA free flap, describing this flap for repair of a soft tissue deformity in the face. The first use of the SIEA flap for autologous breast reconstruction was done by Allen3 in 1989.
Autologous flaps from the lower abdomen have evolved over the years, becoming less and less invasive. The free transverse rectus abdominis musculocutaneous (TRAM) flap, the first abdominally based free flap, requires partialor full-thickness excision of the rectus abdominis muscle. Next came the DIEP flap, which requires only incision of the fascia, without excising any muscle. Next, in 1989, the SIEA flap for breast reconstruction was described, which requires neither excision nor incision of the abdominal wall. This is important, as violation of the rectus musculature or fascia can lead to a decrease in abdominal wall strength and integrity. Studies have shown that the SIEA causes significantly less donor-site morbidity than the DIEP or free TRAM flaps.4,5 The DIEP described by Allen in 1994 has the advantage of a more reliable pedicle than the SIEA flap.
Indications and Contraindications
The SIEA flap is the least invasive option when using an abdominal donor site. However, it can be used only in selective cases when certain requirements are met. This is mostly an intraoperative decision, and if the criteria are not met, the DIEP flap is used instead. We have designed an algorithm for selection of the SIEA flap that has been previously published.6 This algorithm will be discussed at length later in the chapter. Some patients may not be candidates for abdominally based autologous tissue reconstruction. These patients may be better suited for reconstruction with an autologous flap from another donor site, such as the superior gluteal artery perforator (SGAP) flap or the profunda artery perforator (PAP) flap from the posterior thigh, to name just two. If the patient has enough abdominal laxity but does not have sufficient tissue to reconstruct an adequately sized breast, it is possible to add an implant to provide additional volume, or to perform a double (“stacked”) free flap.
Contraindications to the SIEA flap include, first and foremost, patients who smoke. In a previous study, we observed a higher rate of donor-site complication in patients who were current smokers at the time of reconstruction (odds ratio, 15.8; p = 0.016).6 We require patients to refrain from smoking for at least 2 months prior to surgery and for 6 weeks after surgery. Patients with a history of prior abdominoplasty or abdominal surgery with excessive scaring in the flap region, and patients with other medical comorbidities that would hinder flap survival, such as coagulation disorders require careful preoperative medical and radiographical evaluation, and may be poorer candidates for microsurgical breast reconstruction. Lastly, certain intraoperative conditions must be met for the use of an SIEA flap. These will be discussed as part of the aforementioned algorithm.
Anatomy
The SIEA flap is sometimes incorrectly referred to as a perforator flap; however, this description is untrue as the superficial inferior epigastric vessels do not perforate a muscle or septum. The SIEA flap is more correctly termed a direct axial adipocutaneous flap as opposed to the DIEP and free TRAM flaps that are supplied by perforating vessels. The vascular supply for the SIEA flap comes from a subdermal vascular plexus that courses superficially and includes many smaller vessels that originate from the superficial inferior epigastric axial vessels.
In 1975, Taylor and Daniel7 published the preeminent anatomic study of the SIEA. This study found the SIEA to be missing in 35% of the study participants. In the remaining participants, the SIEA origins were examined and found to be variable: 48% of the time the SIEA shares a common trunk with the superficial circumflex artery, whereas 52% of the pedicles had the SIEA originate as a direct branch off of the common femoral artery. In 2011, Piorkowski et al8 conducted a study using computed tomography angiography (CTA) to evaluate the superficial inferior epigastric artery for potential use in an SIEA flap. They concluded that of their patients, 43% had at least one SIEA; however, only 21% had an SIEA of adequate caliber for use in an SIEA flap. Our own clinical experience with donor-site dissection of the lower abdomen for free flap breast reconstruction concurred with the results of these studies, as 42% of our 278 patients lacking an identifiable SIEA. Furthermore, of the 58% with an identifiable SIEA, only 54% of those had a suitable caliber (1.5 mm or greater). SIEA flap selection requires a minimum arterial external diameter of 1.5 mm when measured at the level of the lower abdominal incision. Thus, only 31% of the patients in our study had an SIEA adequate for use in a free flap, which is consistant with the findings of the previous studies.
The origin of the SIEA can be found 2 to 5 cm inferior to the inguinal ligament as it leaves the common femoral artery. As mentioned above, although it may branch off alone in some patients, it often shares a trunk with the superficial circumflex iliac artery. Of note, a variety of other origins have been noted in a small percentage of patients, from the deep femoral artery or even the pudendal artery. The SIEA and its adjacent venae comitantes are generally found running lateral to the lateral row of the deep inferior epigastric perforators. The origin of the SIEA is deep to Scarpa’s fascia; however, as it courses superiorly the artery penetrates the fascia and continues cranially in the superficial subcutaneous tissue. There are two options for venous drainage of the SIEA flap, the two venae comitantes that course alongside the SIEA before terminating into the femoral vein and the superficial inferior epigastric vein (SIEV), which drains into the saphenous bulb. The SIEV usually has a sizable caliber, between 2 and 3 mm; however, it runs medial and away from the SIEA, which causes pedicle inset difficulties and can cause arterial kinking. For this reason the, venae comitantes are usually our vessels of choice and are used beyond the point when they merge together into one vein. The average pedicle length for the SIEA flap can range from 5 to 8 cm with arterial diameters anywhere from 1.1 to 1.9 mm.9,10 The area of the SIEA flap is composed of the lower abdomen that is perfused by the SIEA; however, the lateral aspect of the flap may have some overlapping perfusion from the superficial circumflex iliac artery (SCIA).11–14 The 10th to 12th intercostal nerves provide sensation to the region and can be used for reinnervation if a sensate flap is desired.15
The reliability of tissue perfusion and venous drainage across the midline in an unipedicled SIEA flap has been a topic of great debate in the literature. Some studies have concluded that drainage and perfusion across the midline is quite unpredictable, whereas others have shown that the use of tissue across the midline, in zone III and zone IV, is actually possible.16,17 We will address evaluation of cross-flap perfusion and viability of this tissue later in the chapter.
Preoperative Preparations
Preoperative CTA may be ordered to determine if the SIEA is present and of sufficient caliber.8 The imaging will also help to map the path of pertinent vessels within the flap.
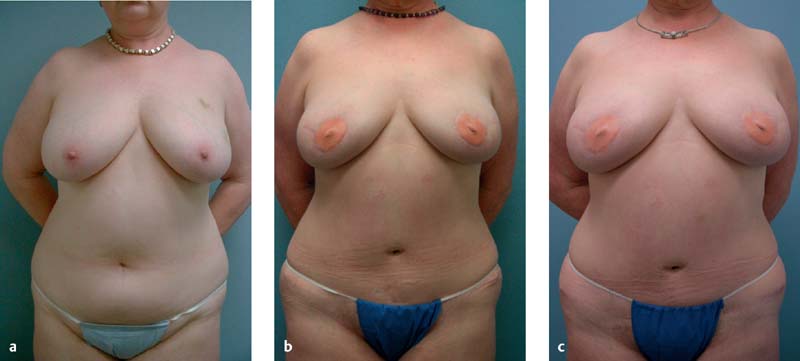
Preoperative marking takes place on the morning of surgery. It begins with marking of the abdomen while the patient is supine, and we mark for the harvest of both an SIEA flap and a DIEP flap ( Fig. 5.2 ). The algorithm for deciding between the SIEA and the DIEP flap occurs intraoperatively.6 All patients have both hemiabdomens marked for possible use of the ipsilateral or contralateral flap for reconstruction.

Marking begins with the use of a pencil Doppler to locate and mark the SIEA and venae comitantes, which are usually located approximately midway between the anterior superior iliac spine (ASIS) and the pubic symphysis, just superior to the inguinal crease. Next, the SIEV is marked, most often medial to the SIEA, followed by the arterial and venous periumbilical perforators bilaterally. At this point, the medial and lateral rows of the deep inferior epigastric perforators are marked.
When marking the inferior incision line, it is important to design this incision low enough to dissect out the SIEA with a suitable diameter. If the diameter fails to meet the 1.5-mm minimum diameter required by the algorithm, a DIEP is performed, which is why preoperative location and marking of the deep inferior epigastric perforators is crucial even when an SIEA flap is expected. The inferior incision mark begins in the midline, immediately superior to the pubic hairline, and extends laterally, with a slight superior curve, terminating at the ASIS. The superior abdominal incision mark begins approximately 1 cm superior to the umbilicus and extends laterally, with a gradual inferior curve, attaching to the inferior incision line at its terminus. The abdomen is then marked down the midline from umbilicus to the mons pubis. The average SIEA flap is 14 cm vertically by 17 cm horizontally from midline to ASIS.
Further marking is continued with the patient standing and depends greatly on the procedure that is scheduled. In patients having immediate breast reconstruction, it is necessary to bilaterally mark the inframammary folds (IMFs) and superior breast poles. Patients undergoing skinsparing mastectomies should also have the anticipated periareolar line marked as well. If the patient is scheduled for delayed unilateral reconstruction, the IMF and superior breast pole markings should match the current contralateral breast; however, in delayed bilateral reconstruction, the “proposed” IMF lines of both breasts should be marked. Previous mastectomy scars should be marked, with all of the aforementioned procedures. Lastly, the rest of the midline is marked from suprasternal notch to umbilicus and the second and third intercostal spaces are palpated and marked for easy identification of the recipient vessels and nerves.
Procedure
Flap Harvest
The patient is placed supine with both arms tucked to her side. This facilitates moving the microscope in and out of the surgical field as needed. While the flap is harvested under loupe magnification x5.5, the microscope is necessary for vessel anastomosis and nerve coaptation in the recipient field. Local anesthetic or vasoconstrictors at the donor site as well as the recipient site are not used.
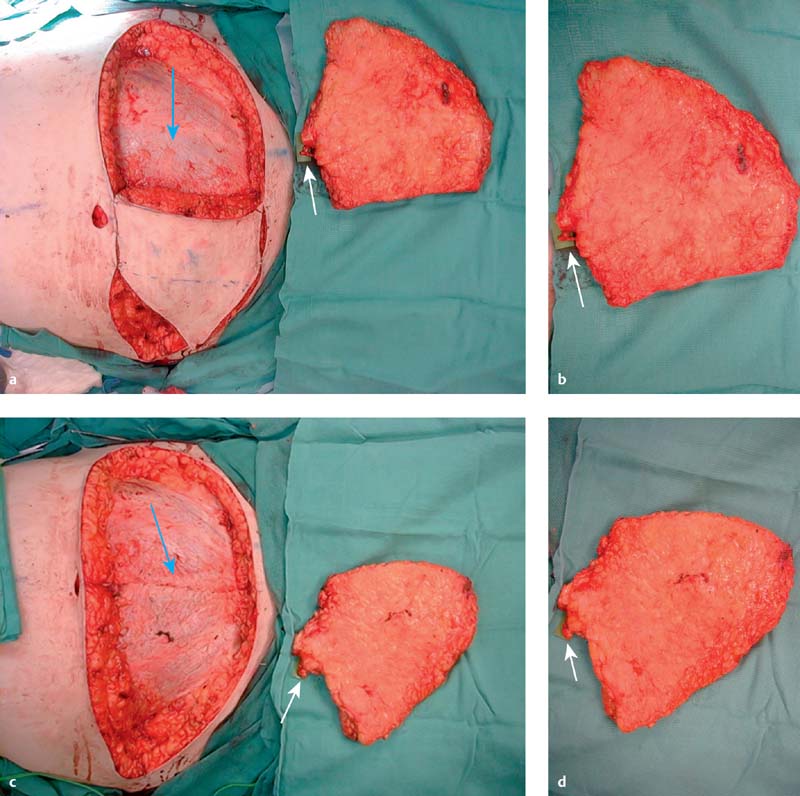
Harvesting the SIEA flap begins on the side ipsilateral to the breast being reconstructed with the inferior abdominal mark. Carefully create an incision along this line just deep to the dermis, and then perform a cautious subcutaneous dissection, making sure not to injure the SIEV, which has a fairly superficial course through this area ( Fig. 5.3 ). Next, locate the SIEA and SIEV and dissect away the adjacent tissue without skeletonizing the vessels. The SIEA should now be evaluated for appropriate caliber at the level of the skin incision.
Before proceeding with the SIEA flap, it is important to use the venous coupler’s vessel sizer to measure the artery’s external diameter. If the vessel meets the 1.5-mm criterion and has a palpable, visible, and audible Doppler pulse, then we will move on to the dissection of the artery and venae comitantes. It is important to continue dissection only as long as the vessel diameter is increasing. There is generally no need to dissect a vessel to its origin. Pedicle length is seldom an issue with the SIEA flap, unlike the DIEP, so there is no need to continue dissection once the vessel diameter becomes constant.* A small amount of subcutaneous tissue or fat deep to the vessels for protection of the pedicle is left around the vessels; however, it should be noted that leaving too much tissue in this area could lead to unnecessary seroma formation. Only the distal end of the vessel should be fully skeletonized, as this is necessary for anastomosis.
For unilateral breast reconstruction, the ipsilateral hemiabdomen is used for three reasons. First, the pedicle of the SIEA enters the abdominal tissue from the lateral border, so when an ipsilateral flap is rotated 180 degrees for inset on the chest, the pedicle will be closer to the recipient vessels on the medial aspect of the chest. Second, when attempting to shape the flap, by suturing an ipsilateral flap around the umbilical excision site, the flap will form a coned shape that sits in the more natural lateral position. Third, the inset position of an ipsilateral flap puts the area with the least reliable blood supply in the least prominent (lateral) position, as opposed to a contralateral flap, which places this at-risk tissue medially, where it is far more visible if it were to necrose. Regardless of the surgeon’s preference of side, both SIEAs are evaluated before pedicle selection, which more often than not is determined by the caliber of the artery. If the caliber is less than 1.5 mm or it shows a weak pulse, the contralateral SIEA will be evaluated. If this contralateral SIEA proves satisfactory, the dissection is continued, and the reconstruction is done with the contralateral SIEA. If neither SIEA is sufficient for our needs, we assume deep perforator system dominance and revert to a DIEP flap. Evaluation for a DIEP flap begins, like with the SIEA flap, on the ipsilateral side for the same reasons mentioned above. The lateral row of perforators is explored first, and then the medial row. If neither is acceptable, the perforators of the contralateral hemiabdomen are evaluated. Bilateral reconstruction similarly favors ipsilateral SIEA flaps over contralateral for all of the aforementioned qualities.
In unilateral breast reconstruction patients who require more tissue than is available in one hemiabdomen to match the contralateral breast, some of the tissue across the midline must be incorporated. Although this is controversial in the literature, as mentioned above, we have seen in our own practice no evidence of increased fat necrosis or partial flap loss with our experience of well over 100 SIEA flaps, as long as the tissue is carefully evaluated for perfusion and nonviable tissue excised before final inset. We have observed reliable perfusion across the midline of an SIEA flap to approximately the lateral row of deep inferior epigastric perforators. Once the flap anastomosis is complete, zone IV and the poorly perfused area of zone III should be resected. Inspection and evaluation of this tissue will be discussed later in the chapter.
Once all the criteria of the algorithm have been met and the decision to proceed with the SIEA flap has been made, the relevant vessels should be identified and flap dissection continued. The superior incision begins at the lateral intersection of the abdominal incision lines marked preoperatively, near the ASIS, and continues medially along this superior marking to the midline. Continue this incision deeply, through the adipose tissue to the loose areolar tissue plane. This tissue lies immediately superficial to the muscular fascia of the abdominal wall. Next, elevate the flap off of the abdominal wall starting laterally and working medially, using Bovie cautery for complete hemostasis. Careful hemostasis is vital at this time to maintain a clear view of the correct surgical plane and prevent accidental incisions into the muscular fascia that can weaken the abdominal wall and increase donor-site morbidity.
Next, use blunt dissection to free the umbilicus from the abdominal tissue. Then elevate the umbilicus with skin hooks and create a circumumbilical incision down to the rectus sheath to free the umbilical stalk, being careful not to skeletonize the stalk, as the surrounding blood supply is necessary for umbilical survival. While this region is exposed, the patient should be evaluated for periumbilical hernias, and any finding should be repaired with your closure and documented.
At this time it is important to test the superficial vascular system to see if it is able to support perfusion to the flap, before continuing. First, compare the recipient artery diameter to that of the SIEA and if there is a difference of more than 1 mm, strongly consider reverting to a DIEP flap. Next, to assess the vasculature, without removing the option of reverting to a DIEP flap, two or three deep perforators from the ipsilateral side should be preserved, and then use vascular clamps to occlude all the deep perforators on both sides as well as the contralateral SIEA and SIEV. At this point the flap is perfused only by the superficial system of the ipsilateral side and we can easily assess the flap for any areas being deprived of perfusion that would most likely not survive flap transfer. Now a decision is made as to whether or not the adequately perfused tissue will provide enough volume to reconstruct the breast, or if a DIEP flap, which generally provides more volume from better profusion across the midline, should be used.
Once flap elevation is completed, mark the superficial side of the pedicle with a marking pen, for future alignment, and then bring the flap edges back together on the abdomen and staple them in place while the recipient site is addressed. If a bilateral reconstruction is planned, the first flap should be anastomosed before evaluating the contralateral SIEA caliber and pulse to determine whether the superficial system is suitable for reconstruction or if a DIEP flap should be considered.
Related posts:
 2 Starting a Perforator Flap Breast Program
2 Starting a Perforator Flap Breast Program
 10 Bipedicled (Double or Stacked) Abdominal Perforator Flap in Unilateral Breast Reconstruction
10 Bipedicled (Double or Stacked) Abdominal Perforator Flap in Unilateral Breast Reconstruction
 9 Pedicled Lateral Thoracic Flap for Breast Reconstruction
9 Pedicled Lateral Thoracic Flap for Breast Reconstruction
 13 Lateral Thigh Perforator Flap (Septocutaneous Tensor Fasciae Latae Perforator Flap)
13 Lateral Thigh Perforator Flap (Septocutaneous Tensor Fasciae Latae Perforator Flap)
 15 Deep Circumflex Iliac Artery Perforator Flap for Breast Reconstruction
15 Deep Circumflex Iliac Artery Perforator Flap for Breast Reconstruction
 11 Venous Salvage Procedures in the Deep Inferior Epigastric Perforator Flap for Breast Reconstruction
11 Venous Salvage Procedures in the Deep Inferior Epigastric Perforator Flap for Breast Reconstruction
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


