49 Local and Regional Cutaneous Flaps
Introduction
Cutaneous malignancies continue to increase in prevalence and represent the largest indication for cutaneous defects of the face and neck. As such, local flaps for facial reconstruction are becoming a significant portion of the otolaryngology practice and a worthy skill to master; it remains a challenging and rewarding part of facial plastic surgery. Over the years, the standard of care has risen significantly, and today’s expectations are an inconspicuous, aesthetic result with preservation of normal function. Many contemporary principles have allowed us to further these goals in our everyday practice.
Cutaneous lesions can be treated in a variety of ways, but Mohs micrographic surgery represents the gold standard for complex malignancies of the face and neck. Frederick Mohs first described this technique in the 1940s while a medical student at the University of Wisconsin. 1 This original fixation technique occurred in situ and required a postoperative slough of tissue, forcing a majority of these defects to heal by second intention. The development of immediate, fresh-tissue fixation allowed the definitive excision to be completed much more quickly and permitted immediate repair, thus opening the door for a growing field in facial reconstruction with flaps and grafts.
It is recognized that the primary risk for cutaneous malignancies is a series of high-intensity, short bursts of sun exposure at an early age, such as children with sunburns. Many adults today, however, grew up in an era when the importance of sun protection was less appreciated; consequently the incidence of cutaneous malignancies continues to rise. Ultraviolet-B (UVB) rays are absorbed at the dermal–epidermal junction and are most responsible for malignant degeneration of epidermal cells. UVC rays are the shortest wavelength and are absorbed by the ozone layer in their entirety. UVA rays penetrate to the deeper dermal layer and are more associated with tanning and causing photoaging of skin.
Anatomy and Physiology
Vascular Supply
The cutaneous vascular network is a unique system with an abundant dermal and subdermal plexus that allows for dependable and versatile random donor flaps. This dermal plexus is regulated by arteriovenous shunts that are controlled by the adrenergic neural supply and function as one of the primary thermal regulators of our body. Skin may also have its arterial supply through an axial pattern based on a dominant artery in the subcutaneous layer. Muscular perforating arteries are also a dependable source to the cutaneous vascular bed. Local perfusion pressure is the driving force for random cutaneous flaps. Critical closing pressure is the pressure whereby capillary vessels collapse and all vascular flow ceases. This is thought to occur between 5 and 10 mm Hg. 2 The concepts of perfusion pressure and closing pressure have challenged the old dogma that random donor flaps require a length to width ratio of 3:1. Studies have now shown this to be a fallacy and that the essential variable for flap viability is the perfusion pressure and vascularity at the pedicle base. 3 This understanding has strongly supported the birth of pedicle flaps and microvascular free flaps.
Skin Lines
Langer’s lines were defined by the way a circular wound takes on an elliptical shape as rigor mortis develops. Langer’s assumption was that skin excisions oriented along the long axis of these wounds resulted in more favorable healing. Clinical experience has shown that this is not always accurate and they appear to conflict with other described skin lines. Today Langer’s lines are of historical interest only. Relaxed skin tension lines (RSTL) are derived from vectors of tension within skin that reflect an intrinsic orientation of tension and relaxation of skin at rest. 4 These properties of skin are defined by the microarchitecture, such as the alignment of elastic and collagen fibers, and to a lesser degree, by the influence of underlying bone and soft tissue bulk. RSTLs are the lines of intrinsic skin tension that appear when the skin is in repose and represent the directional pull on wounds. They have the greatest cumulative effect on wound tension and final healing. The RSTLs are generally parallel to external skin wrinkles but represent a distinct entity from them and occasionally conflict ( Fig. 49.1 ).
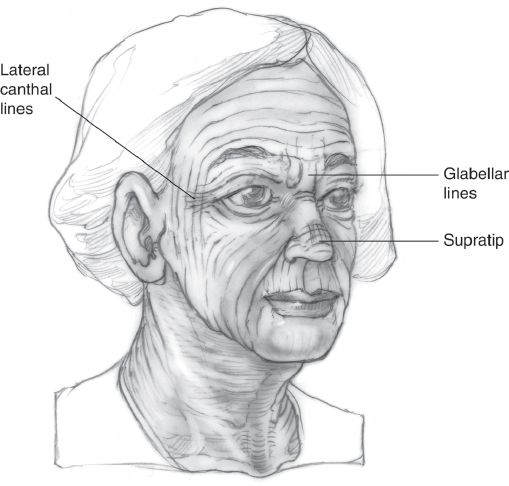
Lines of minimal tension that are also known as natural skin creases or wrinkles are the lines that are externally visible and result from repeated bending of skin from muscular contraction until a permanent cutaneous crease has formed with adhesions between the dermis and deeper tissues. These natural skin creases run perpendicular to muscular fibers and can guide wound orientation for favorable healing. The glabella, nose, and lateral canthal areas have conflicting RSTLs and lines of minimal tension where repeated muscular pull creates permanent skin creases that override the intrinsic tension lines of the skin. In these regions, it is usually best to orient wounds and scars within skin creases rather than the RSTLs for maximal camouflage.
Sleep lines represent the skin creases that result from the patient’s habitual positioning while asleep, where the skin is unnaturally folded and the crease remains independent of the intrinsic skin forces as well as muscular contraction.
Lines of maximum extensibility (LME) are important when recruiting tissue from adjacent areas. The tension on the flap is an essential consideration and can be minimized by studying the LME. These lines typically run perpendicular to the RSTLs and parallel to muscular fibers. Extensibility must be distinguished from elasticity, the latter being the property of recoil as skin returns to its original shape.
Timing of Wound Repair
There is a general surgery dictum that soft tissue wounds that are not closed within 6 hours should be left open to heal by second intention. The rationale for this is the concern over bacterial contamination and subsequent soft tissue infection. Although this is a significant concern with lower extremity wounds, it is not as applicable to the soft tissues of the face and neck. The robust vasculature of the face affords a very low incidence of soft tissue infections, and there is essentially no limit to the delay for facial wound closure. There are occasions where the repair of soft tissue wounds is best delayed for a couple weeks, such as when the accumulation of granulation tissue will improve the contour of the wound bed. Prior to closure of a delayed wound, it should be aggressively debrided with removal of the thin layer of fibrinous exudate that forms on the bed. Wound margins are “freshened” as peripheral epithelialization has often occurred. An important consideration with regard to delayed wound repair is soft tissue contracture, which may be favorable as the overall dimensions of the soft tissue deficit decrease. However, once this contracture distorts surrounding structures, such as eyelids, lips, or the alar rim, its surgical correction can be far more challenging than the original defect.
Wound Care
Closed incisions are cleansed with dilute hydrogen peroxide followed by a thick moisturizing ointment. The purpose of the peroxide is to remove any small blood clots and crusts within the skin incision itself. Left alone, these small scabs may contribute to a slightly wider scar as epithelialization occurs beneath it. Sufficient hemostasis has usually occurred after a few days, and peroxide is no longer needed. Continued moist wound coverage is essential and simple petrolatum gel is sufficient. All open wounds and skin grafts are managed with mild soap and water followed by ointment. Hydrogen peroxide is strictly avoided due to its cellular toxicity and the potentially delayed healing that may occur. Diligent sun protection is critical for at least 6 months following reconstructive surgery and is continually reiterated to the patients. Undermined skin and fresh scars are more sensitive to actinic injury and prone to early tanning and burning. Premature sun exposure may result in a permanent discoloration or a “tattooing” effect on the cutaneous scars.
Flap Nomenclature
Consistent nomenclature of different flaps is important and often overlooked. It expresses a clear understanding of flap physiology and allows for precise communication. Four systems are utilized to characterize flaps.
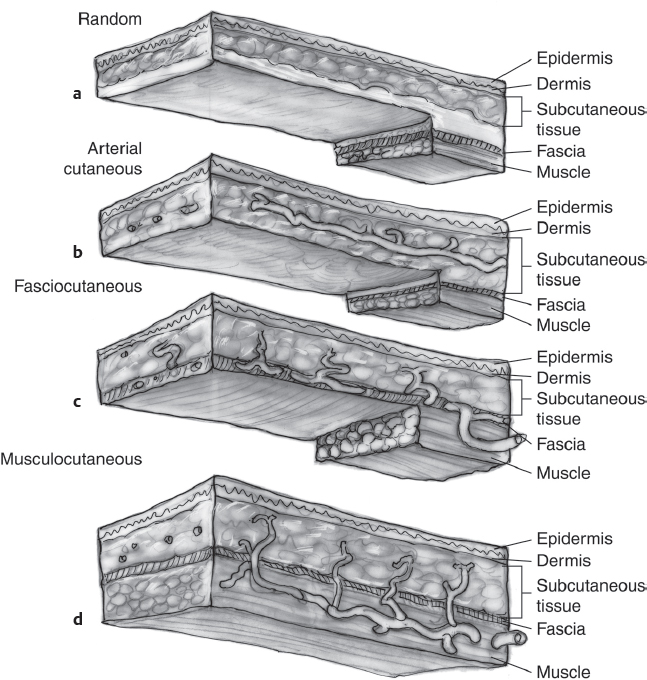
Blood supply. Skin flaps may be characterized by their arterial blood supply as either random donor, axial pattern, or pedicled. The dermal and subdermal plexus alone nourishes random pattern flaps. Axial pattern flaps have more dominant superficial vessels that are oriented longitudinally along the flap axis. Pedicled flaps have larger, named vessels that directly supply the skin paddle, often through muscular or fascial perforators ( Fig. 49.2 ).
Location. The region from which tissue is mobilized is another means of classification. Local flaps generally imply utilizing adjacent tissue. Regional flaps are from different areas of the same part of the body (e.g., forehead flaps for nasal reconstruction). Distal flaps are from different parts of the body, such as a pectoralis myocutaneous flap for the head and neck.
Tissue content. The embryologic layers of tissue contained within the flap or graft are another means of classification. Cutaneous flaps are limited to the skin. As deeper layers are incorporated into the flap they are classified accordingly (e.g., myocutaneous, fasciocutaneous, and composite).
Method of transfer. Method of transfer is probably the most widely utilized system of nomenclature but often inaccurately defined. Advancement flaps are mobilized in a unilinear fashion toward the defect. Rotational flaps pivot around a fixed point and maintain that radius. Therefore, pure rotational flaps are rarely utilized. Most local flaps combine advancement and rotational elements. Transposition refers to a flap that is elevated and mobilized toward an adjacent defect and transposed over an incomplete bridge of skin. A rhombic flap is an example of a transposition flap in that the flap is elevated and transposed over a small triangle of undisturbed adjacent skin. Interposition flaps are similar to transposition flaps; however, the incomplete bridge of adjacent skin is also elevated and mobilized, usually in the opposite direction to fill the secondary defect. A Z-plasty is an example of an interposition flap. Interpolated flaps differ from transposition flaps in that the skin flap is elevated and transferred over a complete bridge of intact skin. By definition, this creates a cutaneous pedicle and mandates a second stage for pedicle division. The forehead flap is an interpolated flap wherein the glabella represents the undisturbed bridge of skin. The island flap is a variation of an interpolated flap where the pedicle is deepithelialized and contains subcutaneous tissue alone. This pedicle can then be buried beneath the intact bridge of skin, thus obviating the second stage. Free microvascular flaps are based on a detached vascular pedicle and transferred to a different region for reanastomosis.
Patient Evaluation: Defect Analysis
During the initial evaluation of a cutaneous defect, the optimal method of reconstruction is not always immediately obvious and an algorithmic method of analysis can assist with flap selection and design. By reviewing four specific areas prior to flap selection, one may lay out the most logical cutaneous flap while avoiding gross facial asymmetry or distortion.
Immobile structures. What are the specific structures relevant to this facial defect that must not be distorted or come under any tension? These include such landmarks such as the hairline, eyelid, melolabial fold, and so forth.
Area of recruitment. Which of the areas surrounding the defect is most readily accessible and has sufficient laxity to allow mobilization toward the defect?
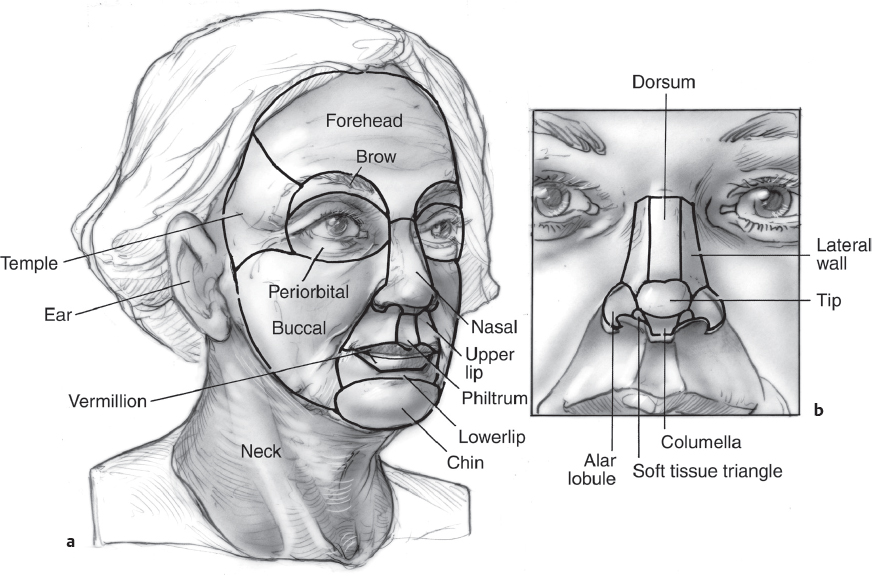
Relaxed skin tension lines and aesthetic units. How are the RSTLs, skin creases, and LMEs oriented in that region to best accommodate additional skin incisions while minimizing wound tension? In addition, the borders of the aesthetic units represent imaginary lines that can accept skin incisions and their subsequent scars in an inconspicuous manner. The principle of the aesthetic unit is based on the fact that our eyes tend to see objects and faces as a series of block images that are spatially organized. For example, the face is characterized by several distinct aesthetic units, each seen by the casual observer as a single block image. The nose has been further divided into aesthetic subunits and has served as one of the major advances in contemporary nasal reconstruction ( Fig. 49.3 ). 5 These aesthetic units of the face and nose are defined by subtle changes in topography, reflections of light, preexisting creases, and transition zones of skin texture. They do not necessarily correlate with the underlying bony and cartilaginous framework. Scars that lie at the junction of two adjacent aesthetic units tend to be inconspicuous because one expects delineation between these facial areas.
Resultant scar. One must always anticipate the final resultant scar of any local and regional flap. Oftentimes these flaps can be oriented in such a way as to comply with the conditions discussed above. Flap design should maximize scar orientation such that they lie within or parallel to wrinkles and/or the borders of aesthetic units.
This algorithm for defect analysis will often lead to the optimal reconstructive flap with the least functional problems and inadvertent distortion.
Second-Intention Healing
Secondintention healing is often overlooked by facial plastic surgeons but frequently employed by dermatologic surgeons and has several advantages. On occasion, secondintention healing may be the method of choice for obtaining the best aesthetic and functional outcome. Wounds that lend themselves to secondintention healing are superficial, concave, and not in close proximity to mobile structures that might be distorted during normal wound contracture. Patients who are exceptionally high surgical risks are also good candidates for this method of repair. A disadvantage of secondintention healing is the length of time required for complete healing; an average 1-cm defect may take close to 4 weeks for total reepithelialization. The inconveniences associated with an open wound often exceed that of a surgical repair. If wound contracture occurs and causes significant distortion to adjacent structures, the secondary repair is often a formidable challenge. Soft tissue contracture usually involves deeper tissues, and a multilayer reconstruction may be needed for correction.
Surgical Treatment
Advancement Flap
When closing cutaneous wounds in general, it is preferable for the edges to bevel away from the center to allow maximal skin eversion during subcuticular closure with the deep, buried sutures. The technique of Mohs surgery leaves wound edges beveled toward the center of the wound, creating a saucer-type defect. Wound edges from a Mohs defect must be “freshened” and rebeveled prior to definitive closure.
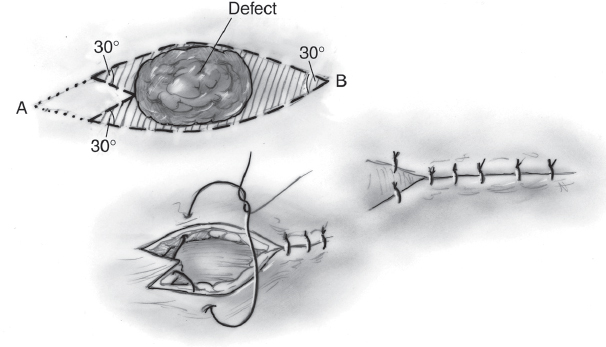
Primary closure is the simplest form of an advancement flap. An advancement flap refers to mobilizing tissue in a unilinear dimension without a rotational element. Circular defects closed primarily must be modified to an elliptical shape to avoid standing cutaneous deformities. The terminal angles of a defect should be roughly 30 degrees or less to avoid this “dog ear” deformity. This 30-degree angle serves as a reference to dictate how far one must extend the ellipse and how much normal tissue will be discarded. When this tissue cannot be readily sacrificed, the ellipse can be converted to a W-plasty with the apices of the “W” 30 degrees or less ( Fig. 49.5 ). This preserves some surrounding tissue and also avoids extension of the resultant scar. A W-plasty can be very useful for cutaneous defects in close proximity to facial landmarks, such as a lower lip defect repaired primarily using an inferior W-plasty to avoid a scar that traverses the mental crease.
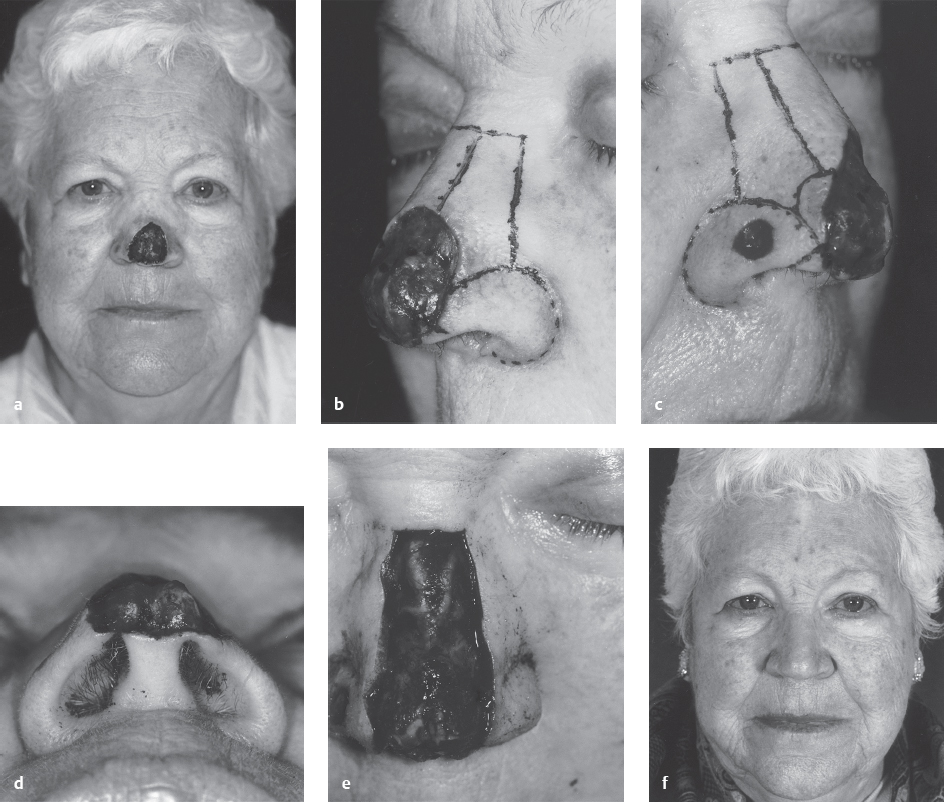
Case 49.1 (Fig. 49.4)
A 62-year-old woman is referred for repair of a Mohs defect of the nose. The 2.5-cm defect involves central the tip and lower dorsum (a). The subunits of the nose were drawn (b) to show the defect involving parts of the sidewall, tip, and dorsum. A smaller basal cell defect was also present in the left alar subunit (c). The base view shows the extent of the tip defect (d). To prepare for a paramedian forehead flap the defect was expanded to include the remainder of the dorsal subunit and a template was drawn (e). Six-month postoperative view after forehead flap and subsequent take down with thinning of the flap (f). Combining subunits such as the tip and dorsum can lead to a more natural contour.
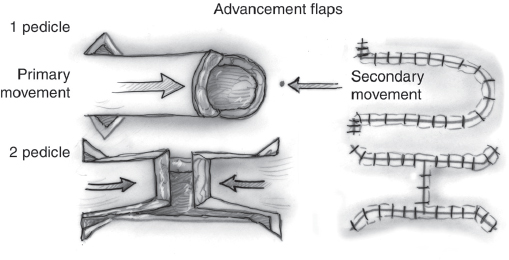
Pure advancement flaps have the feature of limiting wound tension to a single vector with minimal perpendicular tension ( Fig. 49.6 ). Advancement flaps are often utilized in the forehead and eyebrow areas to capitalize on the natural forehead furrows while causing no vertical distortion of the hairline superiorly or the brow margin inferiorly. The skin edges from the flap and nonflap sides are of different lengths, and their closure may create one or several standing cutaneous deformities that may require direct excision (Burrow’s triangles). These excisions create scars perpendicular to the flap margin, which are generally undesirable and should be positioned as inconspicuously as possible. When smaller discrepancies exist, the flap borders may be closed primarily through serial halving sutures; each sequential suture is placed midway along the incision such that the length discrepancy becomes evenly distributed along the length of the wound.
V-Y flaps are also advancement flaps in that they are mobilized in a linear direction. They are based on a subcutaneous pedicle, which may limit the amount of advancement the flap can achieve. The secondary defect is closed primarily and the resultant scar resembles the letter “Y.” Cheek defects along the alar facial groove are amenable to a V-Y flap repair, recruited from the melolabial fold. This minimizes distortion to the nose and upper lip while preserving the general orientation of the melolabial fold.
Scalp Flap
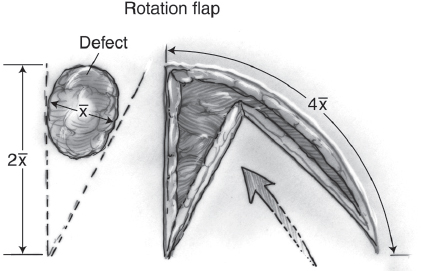
The scalp flap is a unique example of a pure rotation flap due to the extreme inextensibility of the galea in and around the flap. Many facial defects can be closed with a rotation flap designed with an arc four times the diameter of the defect ( Fig. 49.7 ). On the scalp, however, the arc must be roughly six times the wound diameter to allow primary defect coverage. Galeal incisions can improve the extensibility and are best performed parallel to the arterial flow and perpendicular to lines of tension. Multiple rotation flaps can be designed around the primary defect in a spiral fashion. 6 Scalp defects occasionally require preoperative tissue expansion to create adequate coverage. 7 The advantage of using a scalp flap for defects of the head is coverage with like tissue (i.e., adjacent hairbearing tissue). A reasonable alternative is to allow secondintention healing or skin graft coverage followed by serial excisions every 2 months.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


