48 Minimally Invasive Options and Principles for Cutaneous Reconstruction
Principles to Assess Facial Defects
To determine the optimal method for reconstruction, one must fully define the given defect. The defect is defined by the tissue layers that are missing, location, surface area of involvement, and its relationship to the aesthetic subunits.
The initial wound assessment involves determining the size, location, and depth of the facial defect while being cognizant of the possibility that underlying neurovascular or glandular structures might also be missing. Evaluating the depth of the defect (subcutaneous space, facial musculature, cartilage, and bone) is crucial for planning the appropriate repair. By palpating the wound and its surrounding structures, the structural support of the area is determined. If structural support is missing, computed tomography might be helpful in determining if additional underlying support is required. The extent of the tissue loss and orientation of the wound in proximity to surrounding mobile facial structures (eyelids, nasal alae, nasal tip, auricle, vermilion, commissures, and philtral ridges) should also be evaluated.
The major reconstructive goal is to reestablish functional structural support and soft tissue coverage, maintaining the most aesthetic appearance with minimal distortion. Ideally, the absent tissue should be repaired with like tissue that is similar in color, texture, and thickness. Absent supporting structures (bone and cartilage) should be replaced to obtain appropriate projection and contour. Wound healing should be optimized to avoid infection, excessive contraction, and scarring.
Planning Guidelines and Facial Subunits
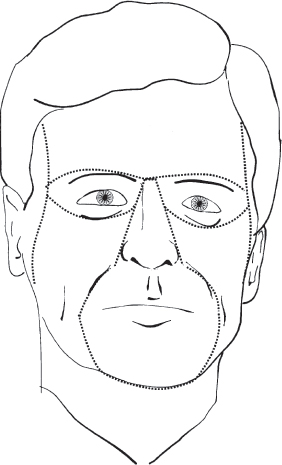
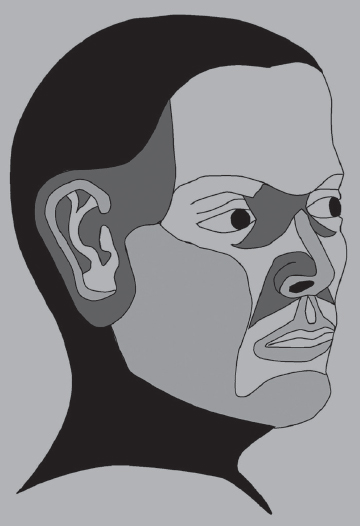
The extent of the missing facial subunits should be evaluated. If the contralateral face is normal, it can be used as a visual template for guidance. Dividing the face into six major facial aesthetic units (forehead, eye/eyebrow, nose, lips, chin, and cheek) is helpful in reconstructive planning ( Fig. 48.1 ). Aesthetic units of the face represent anatomical boundaries, and scars lying on these boundaries appear more concealed. This is because the borders of the aesthetic units are defined by light reflections and shadows of the facial contours. Within some aesthetic units, additional anatomical boundaries can be divided into subunits. This boundary division is applicable to the nose, which can be divided into the subunits—nasal dorsum, nasal tip, columella, nasal alar, soft tissue triangles, and nasal sidewalls. 1
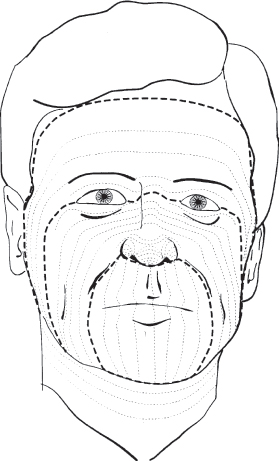
Scars are concealed maximally by adhering to techniques of tensionless wound closure, wound edge eversion, and placement of the closure into relaxed skin tension line (RSTL) of the face ( Fig. 48.2 ) or at the border of facial aesthetic units.
With any wound, the proximity of the tissue loss with respect to nearby mobile facial structures (eyelids, nasal alae, nasal tip, auricle, vermilion, commissures, and philtrum) should be recognized. This is to avoid distortion of these neighboring structures during closing of the wound, which can make the scar much more noticeable.
When a tissue defect cannot be adequately closed primarily without undue tension or vital structure deformity, planning for reconstruction is required. Reconstructive options include healing by second tension, local skin flaps, skin grafts, regional flaps, or free flaps. For wound sites having the majority of a facial aesthetic unit missing, considerations can be made for removal of the remaining aesthetic skin unit followed by local skin flaps or skin grafting. This technique can maintain uniformity of skin color and contour of the facial unit and make scars less visible by having them lie on the aesthetic unit boundaries. For defects encompassing more than one facial aesthetic unit, the units can be reconstructed independent of one another.
Conservative options for cutaneous facial reconstruction are primary closure and healing by second intention. Oftentimes, minimally invasive techniques for facial reconstruction are the best choice in reconstructing facial defects. The first portion of this chapter focuses on these minimally invasive reconstructive options for facial repair. In treating patients requiring facial reconstruction, the major objectives and time course for healing should be carefully discussed with the patient and family so that a mutual agreement is made regarding the reconstructive goals.
Primary Closure
Tensionless closure of each layer (mucosa, muscle, subcutaneous tissue, and skin) should be achieved. To avoid distortion of nearby structures, differential undermining of the wound edges in the subcutaneous plane may be necessary. Differential undermining signifies dissecting in the subcutaneous plane only on one side of the wound. This is performed only to advance the undermined side of the wound edge to avoid distorting the nonundermined side of the wound. The deeper layers can be closed individually with buried absorbable suture to avoid transmitting tension to the skin surface. With dermal closure, eversion of the skin edges can then be performed. To minimize a “trap door” deformity with a beveled wound edge, excessive dermal tissue can be conservatively excised to create a more vertical skin edge. When a defect cannot be adequately closed primarily, other options include healing by second intention, local flaps, or skin grafts.
Most small facial lesions can be excised in a fusiform fashion and a simple closure performed with a good cosmetic result. The key to maximizing this technique is to place the lines of excision parallel to the RSTLs whenever possible. 2
As a result, the maximal tension on the wound is parallel to the lines of maximal extensibility (LMEs). LMEs are usually perpendicular to the RSTLs and represent the direction in which closure can be performed with the least tension. 3
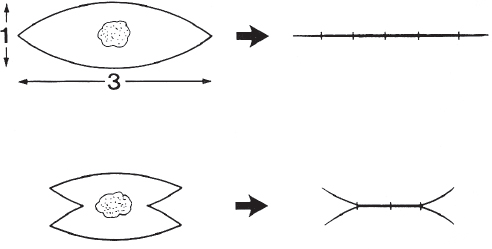
If the surgeon wishes to shorten the total length of the fusiform excision (especially when the fusiform apex > 30 degrees), an M-plasty can be used ( Fig. 48.3 ). The M-plasty is especially useful when the standard fusiform excision would cross from one facial subunit to another or cross a normal facial groove (e.g., melolabial fold). A Gillies corner stitch should be used to close the corner of the M-plasty. This pulls the tips of the M-plasty toward the middle of the incision and prevents skin deformation at the end of the incision (i.e., dog-ear deformity).
Healing by Second Intention
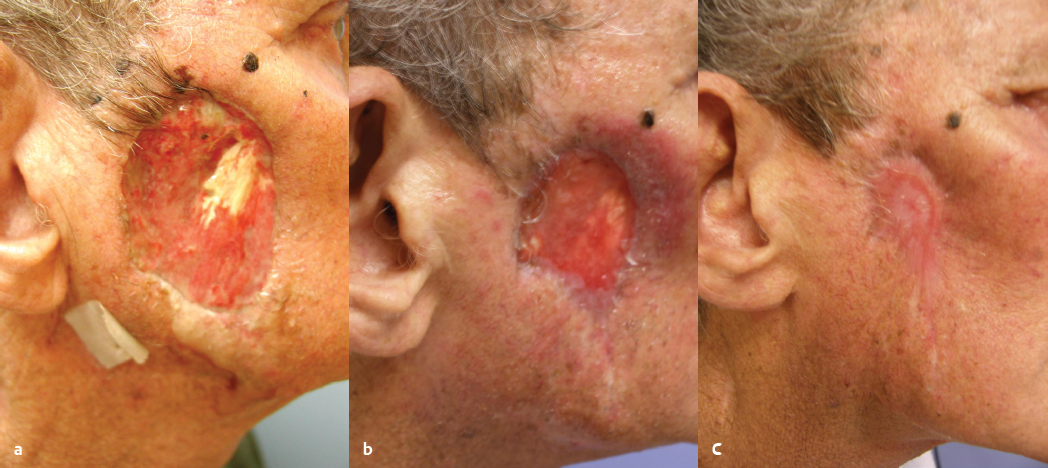
Healing by secondary intention involves the restoration of soft tissue defects by promoting granulation tissue followed by reepithelialization and wound contraction. However, the healing of fullthickness dermal wounds does not transform into an intact layered integument complete with adnexal structures. Hence, secondintention healing results in an appearance and scar texture different from that of normal adjacent skin ( Fig. 48.4 ).
Factors in Considering Second-Intention Healing
Clinical factors to consider when contemplating secondintention healing include the shape and contour of the wound, potential for compromised healing of future flaps or grafts, patient at high risk for local tumor recurrence, patient ill-suited to undergo surgical reconstruction, and a wound requiring a granulation tissue bed for receiving grafts. In addition, a desire to decrease the initial size of large facial wounds prior to reconstruction may give an early option for secondintention healing.
Compromised wound beds occur in persons with previously irradiated skin, in patients with diabetes, in users of tobacco, and in persons with contaminated wounds. Hemorrhagic diatheses may cause hematoma and failure of flaps or grafts while not greatly interfering with secondintention healing. In some case, blood thinning agents—such as aspirin, nonsteroidal anti-inflammatory agents, ticlopidine, heparin, and warfarin—cannot be discontinued, thus making immediate reconstructive options more difficult. In these cases, secondary-intention healing may be preferred.
Despite careful performance of Mohs micrographic surgery, some patients remain at high risk for local tumor recurrence. 4 Such tumors may manifest perineural, perivascular, muscular, cartilaginous, or osseous invasion, or possess an inherently aggressive histopathologic growth pattern. This is especially true of sclerosing, morpheaform, and keratinizing (metatypical) basal cell carcinoma (BCC), poorly differentiated squamous cell carcinoma (SCC), microcystic adnexal carcinoma, extramammary Paget’s disease, and sebaceous carcinoma. In fact, some authors advocate against immediate reconstruction of recurrent basal cell cancers. 5 Reconstruction in such patients may obscure and delay diagnosis of clinical tumor recurrence.
Secondintention healing may effectively aid rather than supplant reconstruction. Deep wounds amenable to fullthickness skin grafting may benefit from filling of the defect with granulation tissue prior to grafting. This approach can reduce graft depression and poor postoperative tissue contour. Large facial wounds healing by second intention may contract sufficiently to make possible delayed reconstruction or create smaller scars than the original. Finally, secondintention healing can be used concurrently with flap or graft reconstruction. Especially in a setting of complex facial wounds involving two or more facial cosmetic subunits, one can select secondintention healing for one appropriate subunit while reconstructing the adjacent one. Use of certain flaps may allow a defect to shift to an area more likely to heal better by second intention. Upper forehead wounds resulting from donor site defects of paramedian forehead flaps used in nasal reconstruction often heal by second intention with very satisfactory cosmesis. Fullthickness skin defects at the posterior auricular sulcus and midhelical rim usually heal with minimal scarring by second intention. 6
Secondintention healing should be given serious consideration for anatomical locations in which excellence in both function and cosmesis are expected. A shortcoming of secondintention healing is poor function when wounds are large or deep and involve or lie in proximity to anatomical free margins, lip, ala, eyelid, and, occasionally, the external ear canal. The process of wound contraction may pull on free margins distorting position and creating dysfunction. Tension on the lip, eyelid, and nasal ala will cause distortion. Defects involving a significant portion of the circumference of the auditory meatus may cause meatal stenosis. Except for these situations, which are prevented by appropriate reconstruction, secondintention healing usually does not result in anatomical dysfunction. Zitelli observed that healing in anatomical sites characterized by concave surfaces (on the nose, eye, ear, and temple—or NEET—areas) produced superior cosmetic results. 6 , 7
Convex surface defects (on the nose, oral lip, cheeks, chin, and helix—NOCH—areas) healed with obvious scars. And flat surface defects (on the forehead, antihelix, eyelids “I,” and remainder of the nose, lips, and cheeks—FAIR—areas) healed with satisfactory cosmetic results ( Fig. 48.5 ). Several other factors contribute to the expected cosmetic result of secondintention healing. The pallor of mature scars stands out more in patients with darker pigmentation (Fitzpatrick types III to VI). In a given anatomical subunit, smaller and more superficial wounds leave less noticeable scars, particularly when the defect retains appendages that re-create the pore pattern of normal skin. Skin with large and numerous sebaceous glands (distal nose, medial cheeks, or in early rhinophyma) are more prone to have visible scarring. 7
Wound Preparation and Care for Second-Intention Healing
We practice the following routine in managing wounds selected to heal by second intention. To optimize wound healing, the tenets listed in Table 48.1 are followed. The patient or caregivers, if available, are involved in initial dressing application. If a significant amount of periosteum is removed, decortication of bone to expose the diploic layer can help promote adequate granulation tissue formation. 8 This may be achieved using a rotating bone bur, rongeur, carbon dioxide laser or an erbium:YAG laser. 9 , 10 Bone exposed in this manner, if not kept moist, may become devitalized and impede wound healing. Hydrogen peroxide should not be consistently applied to exposed bone or cartilage due to its desiccating effects. 1 Wounds with exposed bone should be reviewed regularly to remove devitalized tissue until a complete granulation tissue bed has formed. The presence of significant infection (chondritis or osteomyelitis) in either of these settings is unusual.
Patients are specifically instructed to ensure a moist environment and not to allow dry scabs to form because dry eschars dramatically slow wound healing and contribute to postoperative pain. 11
Wound cleansing is performed and new dressings applied twice daily for the first week, then decreased to once daily until complete healing has occurred. To help determine the kind of dressing to use, Tables 48.2 and 48.3 describe the types of dressings available and their reasons for use.
Wounds are reexamined within a week to judge the adequacy of wound care, provide coaching of technique, and perform surveillance for adverse events. Wound examinations then occur monthly until the wound has healed completely. Once healing has taken place, patients are seen annually, or as dictated by changes in status, for surveillance of recurrence or development of new suspicious lesions. Wounds managed by second intention often heal initially with an indurated, red, or violaceous central papule or ridge. This resolves with time or its resolution may be accelerated by twice daily digital massage with lotion or ointment. Massage enhances blood flow and speeds scar tissue remodeling.
Wound Healing of Second Intention
Wound healing is dependent on the following physiologic steps: hemostasis (occurring over minutes), inflammation (occurring over 3 days after injury), proliferation (occurring from the 3rd to 12th day after injury), and remodeling (occurring over months after injury). In open wounds healing by secondary intention, contraction plays a critical role. All of these components must be present in a coordinated sequence for optimal healing to occur.
When one healing step is delayed, all subsequent healing steps are affected. When one or more of these steps is impaired, delayed healing becomes apparent, resulting in more scarring. Wound remodeling is the last and longest phase of soft tissue wound healing. During this period, granulation tissue recedes, collagen remodels, and a mature scar forms. Scar maturation takes place over years, with gradually increasing tensile strength. However, the strength of healed tissue never reaches that of uninjured skin.
As long as a wound remains open, inflammation persists. This is because in an exposed wound, continual exposure to microorganisms and foreign material acts as an inflammatory stimulus. For inflammation to resolve, this stimulus must be eliminated. The epithelium is the key barrier that protects the wound from the external environment. After a wound becomes reepithelialized, the underlying tissue is further protected and inflammation is curtailed.
It is believed that something in the epithelium suppresses inflammation. Clinically, this is supported by observing that closing a wound primarily or covering a wound with a graft reduces the inflammation. If an open wound fails to reepithelialize within 2 to 3 weeks, the likelihood of a hypertrophic scar developing increases. 12 The use of vacuum-assisted devices has also been helpful to further encourage granulation tissue formation in open wounds. 13
Skin Grafts
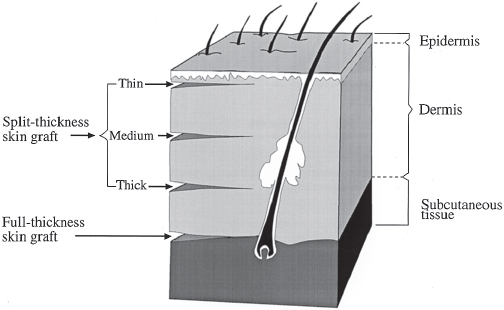
A skin graft consists of a segment of dermis and epidermis that has been completely separated from its blood supply and donor site and transferred to a recipient location. Skin grafts are classified as splitthickness skin grafts (STSGs) and fullthickness skin grafts (FTSGs) ( Fig. 48.6 ).
Skin grafts are often considered when local skin flaps are not feasible. Compared with skin flaps, skin grafts give less optimal color match and texture on the face. STSGs (0.010 to 0.018 inches) can provide temporary coverage of soft tissue defects if adjacent soft tissue viability is uncertain or if a large amount of soft tissue coverage is required. However, they give poorer color and texture match than full FTSGs, giving a lighter, more atrophic, and glistening appearance. They also have less skin durability to infection and to future trauma with increased wound contracture. FTSGs give more acceptable facial color and texture match in comparison with STSGs if they are taken from the preauricular, postauricular, upper eyelid, nasolabial, or supraclavicular donor areas.
When obtaining skin grafts, one should be aware that skin thickness varies with age, sex, and region of the body. Skin is 3.5 times thinner in newborns than in adults. By 5 years old, the skin thickness in children is close to that of adults. Females have thinner skin than males. By body region, skin is thinnest at the eyelids (0.017 inches) and thickest over the soles of the feet and palms (0.150 inches). 14
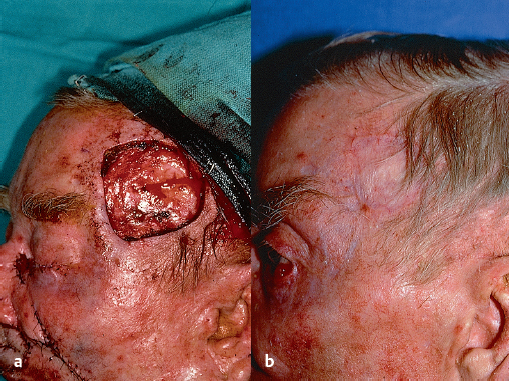
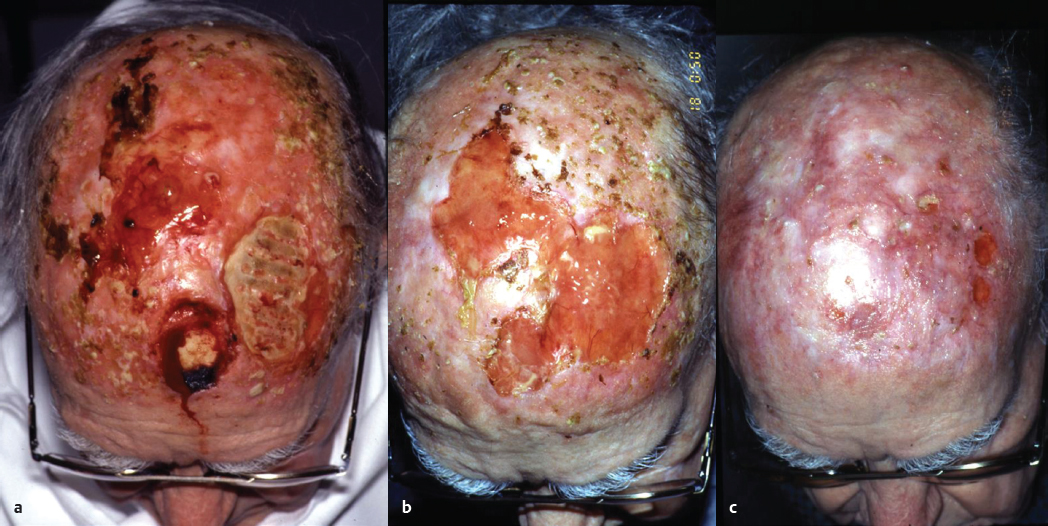
STSGs can be used to cover any wound that has a blood supply sufficient to support its survival. Areas that cannot furnish enough blood supply to a graft are on cortical bone without periosteum, cartilage without perichondrium, tendon without paratenon, nerve without perineurium, and any surface with stratified squamous epithelium intact. In addition, a previously irradiated recipient site has a lower blood supply and results in a decreased “take rate” than a nonirradiated site ( Figs. 48.7 and 48.8 ).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


