46 Nasal Septal Perforation: Prevention, Management, and Repair
Introduction
Closure of nasal septal perforations is one of the most technically demanding and difficult of all nasal surgeries. Septal perforation repair is difficult because the perforation represents a hole in three distinct tissue layers, comprising the right and left septal mucoperichondrial flaps, and the intervening cartilage—all three of which must be distinctly separated and repaired individually. Often the flaps have been attenuated and are difficult to sew closed without further tearing. The larger the perforation, the lower the closure rate, and the more posterior the perforation, the harder it is to close. Many procedures have been described to repair septal perforations. Those that are based on an attempt to stretch the septal mucosa through an advancement flap without adequate mobilization generally fail because the septal membrane is relatively inelastic. Those techniques that have the best physiologic result, highest success rate, and best patient acceptance generally require the use of extensively mobilized bilateral intranasal mucosal advancement flaps with the interposition and anchoring of a connective tissue type of graft. The open or external approach provides the best visibility and access for repair.
Patient Evaluation
Presentation
Patients who are symptomatic with their septal perforation usually present with complaints about crusting, bleeding, whistling if the perforation is small, nasal obstruction if the perforation is large, pain, and/or rhinorrhea. The more anterior the perforation is on the septum, the more commonly the patient will be symptomatic because this area of the nose is drier than the more posterior portions. Sometimes if the perforation is small and especially if it is posterior, the patient will not have any symptoms and the perforation will be found simply on examination by a physician. Large perforations generally cause more symptoms of nasal obstruction because they disrupt the normal separate lamellar flow. 1 The symptom of pain is often more ominous because it suggests the possibility of chondritis, which can occur around the edges of the exposed cartilage at the circumference of the perforation. When the septal wall is violated by a perforation, the normal nasal cycle is disrupted, abnormal flow patterns may occur and turbulent air flow can change normal ciliated respiratory epithelium to dry mucosa, which is often noted by crusting on the mucosa, not just at the perforation site, especially in patients with longterm perforations.
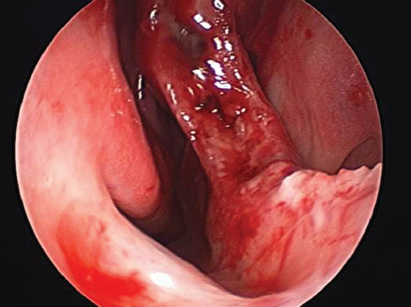
Crusting and bleeding usually occur with septal perforations at the edge of the perforation because of the difficulty for the mucosa to heal over any exposed cartilage ( Fig. 46.1 ). Significant bleeding can occur and must be treated appropriately. In patients with large amounts of crusting, scarring, and inflammation, one needs to consider a chronic inflammatory process and must rule out cocaine abuse or a granulomatous process.
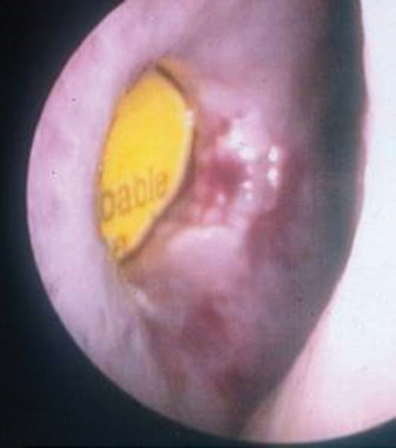
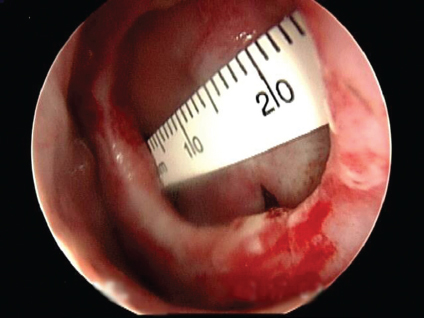
On examination, the septum should be palpated to ascertain if there is any residual cartilage between the mucosal flaps around the perforation site. In perforations after septoplasty, there is usually very little cartilage left around the perforation, and this makes dissection of the adherent flaps much more difficult ( Fig. 46.2 ). Self-inflicted trauma and previous nonchronic cocaine use often leave large amounts of intervening septal cartilage and bone, thus making the repair easier ( Fig. 46.3 ). In patients with granulomatous processes or vasculitis, the intervening septal cartilage is usually of poor quality.

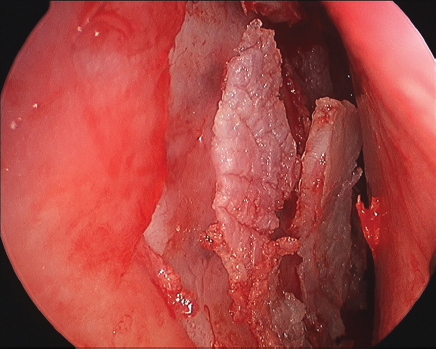
Patients often have no understanding of the complexity of a septal perforation or the difficulty of its repair. A great deal of education is important in helping patients understand that the operative repair is not always successful but is often necessary to restore normal physiology. Showing the patient an endoscopic view of the perforation on a monitor is often helpful in this educational process ( Fig. 46.4 ). 2 , 3
History and Etiologic Factors
Although the most common causes are self-inflicted or iatrogenic, a clear cut etiology must be established from a long list of potential causes, some of which can be life-threatening. A very thorough history and physical examination is necessary in all patients. The septal perforation may be the first sign of a potentially life-threatening generalized systemic process. Table 46.1 clearly identifies the multiple causes of septal perforation, and the reader of this chapter is directed to a previous paper by the author that delineates these etiologies in detail. 4
Trauma |
External Fracture Septal hematoma Piercing injuries |
Self-inflicted Nose picking Foreign bodies |
Iatrogenic |
Nasal surgery |
Septoplasty |
Sinus surgery |
Turbinate surgery |
Rhinoplasty |
Septal cauterization |
Septal packing |
Septal splinting |
Cryosurgery |
Transsphenoidal hypophysectomy |
Postoperative suctioning |
Nasotracheal intubation |
Drugs—legal and otherwise |
Vasoconstrictive nasal sprays |
Steroid nasal sprays |
Cocaine |
Smoking |
Chemical irritants |
Chromic, sulfuric, and hydrochloric acids |
Chlorines and bromines |
Agricultural aerosolized dust |
Chemical irritants |
Rice and grain elevator dust |
Chemical and industrial dusts |
Lime |
Cement |
Glass salt |
Dust |
Heavy metal |
Cyanide, arsenicals |
Neoplastic causes |
Adenocarcinoma |
Squamous cell carcinoma |
Metastatic carcinoma |
Midline destructive granuloma |
Inflammatory causes |
Vasculitides |
Collagen vascular diseases |
Sarcoidosis |
Wegener’s granulomatosis |
Renal failure/renal disease |
Infections |
Tuberculosis |
Syphilis |
Rhinoscleroma |
Lepromatous leprosy |
Rhinosporidiosis |
Multiple fungal species infection |
Mucor infection |
Typhoid |
Diphtheria |
Iatrogenic Causes
Unfortunately, the most common cause of a septal perforation stems from previous nasal surgery, especially after a septoplasty, and from septal cauterization for epistaxis. During septoplasty, there may have been rips or tears in both septal membranes in a contiguous area where the intervening septal cartilage or bone has been removed. If these are not repaired with suturing immediately at the time of surgery and if nothing is placed back between the flaps such as crushed cartilage, the contraction of healing itself may pull apart the rips and a hole can form between the two tears. It is unwise to believe that a perforation will heal on its own; in fact, it is more likely that the perforation will enlarge postoperatively with the contraction of healing. Not only should the membrane tears be repaired but the insertion of an intervening cartilage or connective tissue graft as a barrier to perforation is prudent. 5 The author, when performing a septoplasty, always places crushed cartilage between the septal flaps in the area where the cartilage has been removed, whether or not there have been tears in the septal membranes. Often the obstructing cartilage that is removed during septoplasty is discarded or sent to pathology. Placing it back between the flaps, after it has been straightened or crushed, makes it act as a barrier against perforation and may strengthen areas that have been weakened by the removal of cartilage ( Fig. 46.5 ).
The secret to preventing corresponding tears in both mucoperichondrial flaps during septoplasty is to undermine broadly and elevate the mucoperichondrium away from the deviated cartilage or septal spur areas prior to attempting to remove the spur or the deviation. Even when there is a large spur, where penetrating the overlying membrane is common, the opposite mucoperichondrium usually can easily be elevated first and maintained intact. If only one membrane is torn, the chance of a throughandthrough perforation is markedly decreased. When a large posterior bony spur is encountered, the cartilage is separated from the bony septum and then the mucoperichondrium is elevated over the bony portion of the spur on the opposite side of the spur prior to removal. Becker scissors are used to cut above and below the bony spur, and then the tip of the nasal speculum is used to push the intervening spur closer to the midline as one teases the mucoperichondrium off the protruding portion of the spur prior to its removal.
Bilateral corresponding tears in septal membranes can still cause a septal perforation, even if there is intervening cartilage left; therefore, these tears should be repaired. The blood supply to the cartilage comes from the overlying mucoperichondrium, and if this is disrupted bilaterally the intervening cartilage may necrose and ultimately perforate.
Nasal Sprays and Cocaine Usage
Some steroid nasal sprays can be very irritating to the septal mucosa when used on a longterm basis and can lead to perforation. 6 It is the obligation of the physician who places patients on such sprays to periodically examine the nasal mucosa for any untoward effect of the medication.
Cocaine use has increased dramatically as a major cause of septal perforations. The drug itself causes intense vasoconstriction, compromising blood supply to the flaps. As most street cocaine is adulterated with filler substances that can be quite irritating, such as borax or talc, the insult to the septal membrane can be even worse, and even one-time usage of intranasal street cocaine has been known to cause a septal perforation. 7 Chronic cocaine use can totally destroy the inside of the nose because quite often infection complicates the inflammation, irritation, and decreased blood supply. The necrosis can proceed not only to perforation but also to total nasal collapse, dorsal saddling, intranasal stenosis, and scarring. Because cocaine is so addictive, patients often need to be screened for continued use despite their denial of continued use. It would be useless to attempt to repair a septal perforation in a patient who is still using cocaine.
Disease Processes
Septal perforations can be the sequelae of serious systemic diseases, whether they are neoplastic, inflammatory, or infectious. When no obvious cause has been determined, the physician must rule out potential serious medical illnesses. Renal failure and renal disease, vasculitides, Wegener’s, and collagen vascular disorders such as lupus, rheumatoid arthritis, and polychondritis can predispose to septal perforation. Unfortunately, some of these latter conditions may recur following remission. Therefore, prior to repairing such perforations, it is important to touch base with the primary physician who is treating the patient. Patients with these disorders must be told that even though repair may be successful, recurrence is possible if the disease flares up again at a later date. The author has noted this in several patients with renal and small vessel disease. 8 Wegener’s granulomatosis, sarcoidosis, and other granulomatous diseases are less common causes, but computed tomography of the nose and paranasal sinuses helps to rule out these conditions. The workup of individuals with no known cause and a negative head and neck examination, and negative computed tomography scans, should include laboratory evaluation for collagen vascular and renal disease. It should also include fluorescent treponemal antibody, absorbed, Venereal Disease Research Laboratory, cytoplasmic antineutrophilic cytoplasmic antibody, and Epstein-Barr virus titers. Nasal cultures for fungi and bacteria are helpful in the presence of any inflammatory process. Skin testing for anergy, tuberculosis, and fungal infections may also be helpful. If all of these tests come up negative and no clear cause has been elicited, then a biopsy of the perforation may be indicated. Such a biopsy should be taken from the posterior edge of the perforation and should be large enough to include tissue away from the perforation so that the pathologist can get a definitive diagnosis and just not render a report of chronic inflammation. It is important not to biopsy at the superior or inferior edge of the perforation where one would increase the vertical perforation height, which is the dimension of the perforation that is most critical in one’s ability to close a perforation. In addition, biopsies at the anterior portion of the perforation should be avoided because that area must be closed preferentially to decrease symptoms.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


