45 Reconstructive Surgery of the Nasal Septum
Introduction
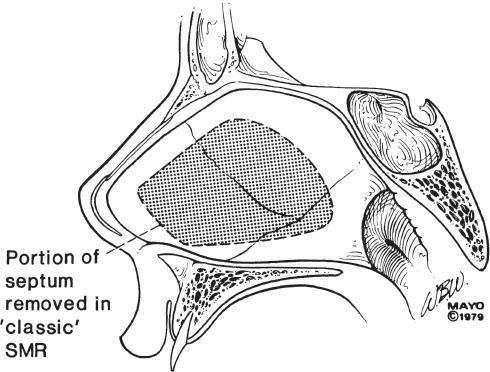
Historically there have been many approaches to the surgical correction of the nasal septum. Prominent 19th century rhinologists, including Bosworth, Roe, Watson, Gleason, Asch, and Douglas, utilized a variety of techniques to address nasal septal deformities. 1 The most common approach was that of Bosworth, 2 who employed a saw to remove the deformity and preserved one side of the septal mucosa. Septal perforation was a common complication. Watson 3 described an early septoplasty technique with preservation of mucosa, and Asch 4 introduced cartilage modification techniques. The 20th century in rhinology opened with the development of the submucous resection technique. Freer 5 and Killian 6 introduced the concept of submucous resection, which allowed relief from a septal obstruction without sacrifice of mucosa. Briefly, an incision is made in the respiratory mucosa 1.5 to 2 cm behind the columella. The incision is carried through the cartilage, and subsequent elevation of mucoperichondrium in a posterior direction on each side of the septum allows removal of obstructive septal structures ( Fig. 45.1 ). Closure is accomplished by mattress stitch approximating mucoperichondrium. Precepts associated with the submucous resection dictate preservation of a dorsal caudal strut of ∼1 cm of cartilaginous septum. Although the submucous resection was a significant advancement, several shortcomings were noted ( Table 45.1 ), with a significant problem involving the inability to address caudal end deformities. Metzenbaum 7 and others 8 , 9 , 10 , 11 , 12 proposed alternative methods for addressing management of caudal end deformities.
|
|
|
|
|
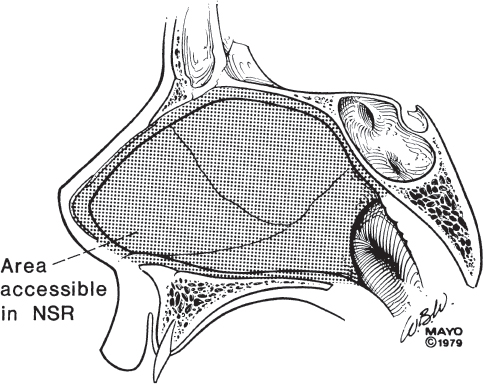
Modern reconstruction surgery of the nasal septum is based on principles forwarded by Maurice Cottle 13 and provides a method to address the nasal septum in a comprehensive fashion. When compared with the submucous resection, the incision is placed through skin (i.e., stratified squamous epithelium rather than respiratory mucosa) and is located at the distal end of the quadrangular cartilage. This subsequently allows access to all borders of the bony and cartilaginous septum ( Fig. 45.2 ). Cottle termed this the maxilla–premaxilla approach. 14 Basic principles formulated with this approach include preservation of mucosa, repair of mucosal tears experienced during the dissection, avoidance of circumferential incisions, and replacement of bony and cartilaginous fragments to reconstruct the septum. This is the approach favored by the authors and described in some detail subsequently. The major advantages are significant and include mobilization of the entire septum when necessary and preservation or replacement of the caudal septum. Realistically, practicing rhinologists use their knowledge of both procedures when operating on nasal septal deformities. Rhinologic innovation in the late 20th century included endoscopic approaches to paranasal sinus disease and, subsequently, endoscopic septoplasty. 15 In this situation, endoscopic equipment in use for paranasal sinus surgery is utilized to complete a submucous resection of limited septal deformities. This technique promotes teaching when video monitors are used, avoids the use of a headlight, and minimizes mucoperichondrial flap dissection.
Nasal septal surgery has evolved as knowledge of the anatomy, physiology, and pathophysiology of the nose has become better understood. Rhinomanometry has significantly advanced the understanding of nasal physiology and pathophysiology while providing objective pre- and posttherapy data. 16 This information has led to a confirmation of the importance of the anterior septum, nasal valve area, and mucosa (turbinates) in nasal respiration, 17 , 18 regulating air flow, and mass transfer. 19 The structures in the nasal valve area (valve angle, septum, anterior inferior turbinate, and anterior floor of nose) require careful investigation. This dynamic area requires a straight, stable septum and an appropriately flexible upper lateral cartilage that provides variable resistance, such as a Starling resistor. 20 Thus, combined with the maxilla–premaxilla approach, rhinomanometry and an understanding of nasal physiology allow the rhinologic surgeon to selectively address septal, mucosal (turbinates), and nasal valve pathologies, thereby improving patient care.
The most common application of the maxilla–premaxilla approach is in addressing caudal septal deformities, which result in airway obstruction. The true flexibility and potential wide exposure of this approach enable incorporation with open and closed rhinoplasties and utilization as a method of midline exposure of the sphenoid sinus (e.g., transseptal transsphenoidal pituitary surgery). In addition, this approach allows mobilization of the septum to allow adequate exposure of the lateral wall of the nose when septal deviations limit exposure to the ethmoids.
Preoperative Evaluation
Patients with disturbed nasal physiology require a complete history, a careful clinical examination, laboratory tests, and a frank discussion prior to surgical intervention. The nose plays a key role in active breathing and ultimately in oxygen and carbon dioxide exchange at the alveoli (respiration). Disturbances of respiration can have far-reaching somatic and psychological effects. A major diagnostic goal is to determine whether the patient’s disturbed physiology is related primarily to a mucosal disturbance, a structural abnormality, or both. If the history suggests a mucosal component to the patient’s complaints such as that caused by chronic inflammation seen in allergic rhinitis or chronic rhinosinusitis, then appropriate medical therapy should be initiated and improvement evaluated following an adequate therapeutic trial prior to addressing structural abnormalities. Topical nasal steroids and topical and oral antihistamines have been shown to be effective in the treatment of rhinitis. 21 The key elements sought in the history are the symptoms of allergic and nonallergic rhinitis, chronic and acute sinusitis, topical nasal decongestant abuse, use of hypertensive medications, and a history of hypothyroidism or pregnancy. These are but a few of the causes of mucosal abnormalities that can produce disturbed nasal physiology and nasal symptoms.
Historical points that may be significant include a history of congenital abnormalities predisposing to structural defects, such as a cleft lip or cleft palate deformity, Binder’s syndrome, or septal trauma with dislocation. Inflammatory diseases, which may produce structural abnormalities, include Wegener granulomatosis, sarcoidosis, and syphilis. A history of trauma is common but important to note, as is a prior history of rhinologic surgery. Certainly, the history suggestive of any neoplastic process is important to note preoperatively, as is a history of sleep apnea. Keep in mind that patients with atrophic rhinitis may present with a complaint of nasal obstruction, and patients with overzealous turbinate surgery seem to present with complaints related to abnormalities in mass transfer (dry, crusted, congested nose; bleeding and pain may be part of the clinical picture).
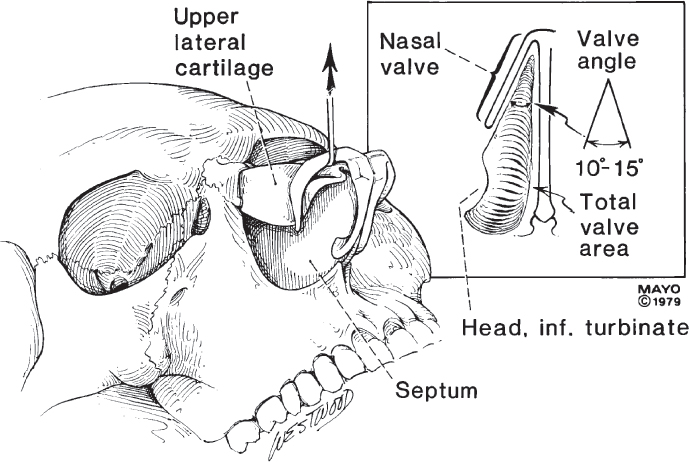
In addressing structural abnormalities that may be associated with disturbed air flow, it is important to assess the location of the septum and its upper lateral cartilaginous extensions as well as the structure and position of the lower lateral cartilage, the nasal valve area, and the lateral nasal wall (especially the head of the inferior turbinate) ( Fig. 45.3 ). The size of the inferior turbinates should also be noted as they can contribute to nasal obstruction. Examination of the patient’s nose should then be correlated with his or her history. The rhinologic examination should include notation of any external deformities. The caudal end, including the valve area, must be carefully evaluated, as this is the most common site of symptomatic septal deformities. This may require utilization of either a pediatric nasal speculum or a fourpronged retractor to allow visualization of the vestibule and nasal valve area with minimal distortion. The position of the septum should be evaluated in relationship to the lower lateral cartilage, the nasal spine, the premaxilla, and the remainder of the nasal valve area. Both the internal and external nasal valve should be assessed. The external nasal valve is the first area of resistance and consists of the area of the nasal vestibule under the nasal ala formed by the caudal septum, the alar rim, and the medial crura of the alar cartilages. The internal nasal valve is comprised of the dorsal septum, the caudal border of the upper lateral cartilage, and the anterior aspect of the inferior turbinate. A modified Cottle maneuver with an ear curette to support the upper lateral cartilage should be performed with any subjective improvement in nasal airflow noted. As depicted in Fig. 45.3 , the normal valve angle is 10 to 15 degrees. This examination should be done prior to and following decongestion. After a thorough visualization of the nasal cavity, it is often beneficial to use a rigid or a flexible endoscope to further assess the mid- and posterior portions of the nasal cavity. This can be easily done following topical application of 1% phenylephrine hydrochloride (Neo-Synephrine). Midseptal deformities can frequently be noted and generally are asymptomatic from an obstructive standpoint. However, they may present with a history of facial pain or a predisposition to recurrent sinusitis.
Sensitive, specific, costeffective, and reliable tests of nasal function would ideally quantify abnormal nasal physiology and confirm response to treatments. Today the documentation of many nasal functions remains elusive or impractical for most facial plastic or rhinologic surgeons. Pertinent to nasal septal surgery, measures of respiratory and olfactory function are available but problematic. The tools readily available for the measurement of olfaction include the University of Pennsylvania Smell Identification Test (UPSIT) and commercially available odorants used in an individualized fashion. Threshold detection testing is complex, timeconsuming, not readily available, and not considered further in this review. The UPSIT is an easily administered forced-choice test based on microfragrance samples from the 3M Company. The test consists of scratch-and-sniff methods of odorant presentation and interpretation based on data from a large number of individuals with “normal” olfactory function. Results from the UPSIT are scored from 0 to 40, with higher scores representing greater olfactory function. Tables are provided that allow scoring of an individual’s result as a percentile of the normal population. Scores can also be categorized into normosmia, microsmia (decreased but not anosmic), total anosmia, and probable malingering. It is difficult to interpret results at age extremes in part due to the sample size and score variability in the normal population studied. Currently this kit called UPSIT is available from Sensonics, Inc.
The utility of olfactory testing is easily recognized when a patient who has had nasal surgery presents with the complaint of decreased olfactory function. Mechanisms responsible for olfactory injury from nasal surgery include direct trauma to the olfactory epithelium, traction on the olfactory nerve due to cribriform plate motion, vascular compromise of the olfactory neuroepithelium during surgery, drug effects, atrophic rhinitis due to excessive removal of intranasal tissue, mucosal edema due to or exacerbated by surgical trauma preventing odorant access to the neuroepithelium, and idiopathic development of anosmia in the postoperative period. Kimmelman 22 utilized the UPSIT to study 93 patients before and after nasal surgery to identify the risk to olfaction. Thirty-four percent of patients scored lower on the UPSIT postoperatively, with a mean decline of 2.25 correct responses resulting in a decline in percentile rank of 25 percentile points. In the group of patients studied, 1.1% developed total anosmia postoperatively and 66% either improved or were unchanged.
Olfactory testing is not routinely performed for patients undergoing nasal and paranasal sinus surgery because it adds time and cost. However, the utility of routine olfactory testing becomes clear when the surgeon is faced with a disturbed patient who reports altered olfaction following nasal surgery.
Rhinomanometry provides objective information regarding the respiratory function of the nasal airway. Rhinomanometry quantifies nasal air flow and pressure, allowing calculation of airway resistance. Three methods exist to measure air flow based on the location of the pressure catheter. Anterior rhinomanometry relies on a catheter placed in a sealed nasal vestibule to measure pressure changes in the opposite side of the nose. Posterior rhinomanometry involves peroral placement of a catheter in the oropharynx, which allows both sides of the nose to be measured simultaneously. Pernasal rhinomanometry requires passing a pressure catheter transnasally to the nasopharynx. This is similar to posterior rhinomanometry, which provides simultaneous measurement of flow and pressure from both sides of the nose. In each method, the patient either wears a mask or is in a chamber that allows measurement of pressure and air flow changes related to breathing. Posterior rhinomanometry requires the greatest degree of patient education and has the highest rate of test failure. Pernasal rhinomanometry causes some irritation with the catheter placement but provides the most consistent results. 23 Anterior mask rhinomanometry is the most common method because it requires the least patient cooperation and has the least complicated equipment.
Data gained from rhinomanometry include the simultaneous pressure and flow of nasal respiration, which are nonlinear during the respiratory cycle. Although a variety of results can be computed, nasal resistance (pressure/flow) is most commonly reported. However, resistance varies at different points on the pressure–flow curve due to the nonlinear relationship. A consistent point on the pressure–flow curve must be selected to allow comparison between tests in the same patient as well as among patient groups. It is important to report the nasal resistance at a given pressure (150 Pa) 24 and at a given radius. 25 Additional parameters that can be reported include maximal nasal resistance 26 and mean resistance. 27 Both maximal and mean resistance can be calculated for all patients, which is advantageous over measuring resistance at set points along the pressure–flow curve because some patients require a voluntary increase in ventilation to reach these points. The challenge for any data gathered from rhinomanometry is variability as well as correlation with clinical symptoms. Some variability is due to nasal sources and includes variable mucosal congestion from exercise, postural changes, pressure applied to certain body areas, nasal secretions, and the nasal cycle. Medications, height, anthropologic type, and age may also induce variability. Methodologic sources of variability include mask leakage, equipment repositioning, and inadequate equipment warm-up. Factors that minimize variability include symmetrical patient sitting position, avoiding exercise 30 minutes prior to testing, consistent temperature and humidity, avoidance of medications prior to testing, and alleviation of patient anxiety by appropriate explanation of the testing procedure. 28
Acoustic rhinomanometry is a method of measuring the crosssectional area of the nasal cavity as a function of distance from the nostril. This technique requires a sound generator, wave tube, microphone, nosepiece, and computer. The sound generator produces an acoustic signal (pulsed or continuous) that travels down the wave tube into the measured object. The sound waves are partially reflected by narrowings in the measured object, thereby representing a change in the crosssectional area. A microphone measures the transmitted and reflected sound, which is digitized with reconstruction of the impedance and area profile plotted as a function of area versus distance. These calculations are based on several assumptions. First, the measured object is a series of cylinders of the same length. Second, there is an infinite signal-to-noise ratio. And third, significant wall inertia exists. All of the above assumptions can contribute to inaccuracies in the measurement of crosssectional areas. Despite these limitations, accurate measurements can be obtained and have been confirmed by a variety of models. 29 A critical portion of the apparatus to measure acoustic rhinomanometry is the nosepiece. The nosepiece must form an acoustic seal with the wave tube and nose yet not distort the nasal tip/valve region. Nosepieces of different shapes and materials yield different data values when the same object is measured. It is best to use nosepieces that are composed of the same material and that are anatomically conformed to obtain accurate measurements.
The results from acoustic rhinomanometry represent the crosssectional area (cm2) of the nasal cavity as a function of distance (cm) from the end of the nosepiece. The data from acoustic rhinomanometry in normal individuals can vary with race, craniofacial development, mucosal variations, environmental conditions, and skeletal variations. Data from acoustic rhinomanometry reveals an initial decrease in crosssectional area related to the narrowing in the region of the nasal valve followed by a subsequent narrowing due to the anterior head of the inferior turbinate. These constrictions are typically noted at ∼1.3 and 3.6 cm from the nosepiece. The crosssectional area distal to the head of the inferior turbinate gradually increases to the region of the nasopharynx. Acoustic rhinomanometry should be performed with the patient in a comfortable, symmetrical sitting position before and after decongestion. Several studies have reported the results on normal individuals and patients with allergic rhinitis, vasomotor rhinitis, and patients before and after septal surgery. 30 , 31 , 32
Although acoustic rhinomanometry provides data on the crosssectional area of the nasal cavity, it does not detail the shape of the airway. Therefore, acoustic rhinomanometry cannot provide information on nasal airway resistance. Rhinomanometry determines overall nasal patency but cannot provide information about the geometry of the airway. One can conclude that these are complementary methods of investigating key elements of the nasal airway. The utility of rhinomanometry and acoustic rhinomanometry is limited by the potential need for both studies, equipment-related expense, lack of reimbursement, and test variability. Routine use cannot be mandated, but the benefits are realized in the context of complex procedures or potentially litigious patients.
In 2004 a new technique, optical rhinometry, was introduced which measures the absorption of visible and nearinfrared light in tissue. 33 This technique works similar to the way that pulse oximetry measures hemoglobin absorption of nearinfrared light in order to assess blood volume within the nasal cavity. An emitter and detector are placed over the nasal dorsum and swelling is calculated as the extinction of light or optical density. Recent studies have shown that this technique correlates with acoustic rhinometry in patients undergoing nasal provocation testing. 34 The utility of this test in surgical patients has yet to be determined.
The final aspect of the preoperative assessment consists of discussing the findings of the history, physical examination, and laboratory studies, including the etiology of the disturbed nasal physiology and the planned therapeutic approach. This includes a frank discussion regarding alternative therapies, potential complications, an estimate of the likelihood of success, and, if surgery is required, postoperative recovery time and possible reoperation.
Surgical Technique
The outlined approach to reconstructive surgery of the nasal septum is based on the following precepts and concepts. First, the goal of surgery is to remove pathology and reconstruct the abnormal septal parts into normal position so that normal physiologic airway function can take place. Second, the aim of the incisions and subsequent dissection is to completely expose the pathologic septal structures. Third, the mucosal lining is the valuable organ of the nose where the defense and biochemical reactions occur and incisions should be in the skin to preserve the integrity of the mucosa. Fourth, the goal of surgery is to help relieve the patient of symptoms that distort his or her wellbeing.
Positioning on the operating table for nasal surgery should provide comfort for both the patient and the surgeon. The patient should be placed on a well-padded table or chair (dental flexible chair) as close to the right side of the table as possible to minimize the distance the surgeon must reach to address the nose. A semi-Fowler’s position is frequently used to aid in patient comfort. Recent studies have shown that total blood loss and surgical field visualization (Boezaart endoscopic field of view score) is improved at the 15- and 20-degree reverse Trendelenburg position in the performance of endoscopic sinus surgery. 35 , 36 This could be extrapolated to septoplasty as well as the same physiologic principles of endonasal surgery apply. Two power surgical loops are very helpful in the performance of this delicate surgery.
Nasal septal surgery can be performed under either general anesthesia or local anesthesia with intravenous sedation. Premedication should include analgesics and sedatives. In either situation, the nose is infiltrated with a solution containing epinephrine. The concentration of epinephrine varies; in general, a concentration of 1:100,000 is safe. The solution should be injected in the areas to be approached surgically and additionally focused in areas of incisions and vascular areas. Therefore, areas that are generally infiltrated include that of the hemitransfixion incision between the medial crura, the region of the incisive foramen, the heads of the inferior and middle turbinate (to allow decongestion and increased visualization of the nose), and the region between the upper and lateral cartilage and lower lateral cartilage near the intercartilaginous incision. The external cartilaginous and bony pyramid of the nose is also anesthetized at a similar time. Frequently, 5 cm3 is adequate to accomplish this. It is often advisable, especially under local anesthesia with intravenous sedation, to first spray the nose and vasoconstrict with 1% phenylephrine hydrochloride and then topically anesthetize the nose by spraying two or three puffs of 4% lidocaine. Subsequent application of ∼100 to 150 mg of cocaine flakes on cotton carriers directly to the region of the anterior ethmoid nerves and sphenopalatine ganglion provides excellent anesthesia. Halothane, enflurane, and isoflurane are commonly used inhalation anesthetics. These agents and cocaine sensitize the myocardium to the actions of the sympathomimetics. 37 Therefore, the combination of these agents with the infiltration of an epinephrine-containing solution requires careful cardiac monitoring and minimal dosages of cocaine and epinephrine.
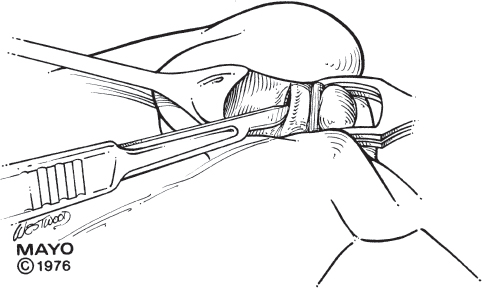
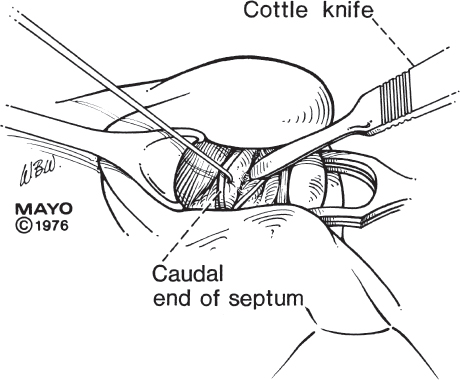
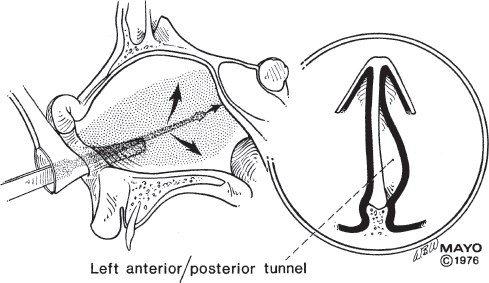
The opening incision for septal surgery is the right hemitransfixion incision ( Fig. 45.4 ). The hemitransfixion incision extends from the anterior part of the caudal end of the septum to the area just anterior to the nasal spine. This incision parallels the caudal end of the septum in the skin. Instruments used to expose the caudal septum and identify the caudal end of the septum include a Cottle clamp and an alar protector. For a more advanced surgeon, a nasal speculum may be all that is required. After the caudal end of the cartilaginous septum is isolated, the elevation of the mucoperiosteum from the left side of the septum or left anterior tunnel is begun ( Fig. 45.5 ). It is important to obtain a dissection plane between the cartilage and perichondrium to maintain the vascular supply to the perichondrium. Several instruments are helpful in this dissection. Selection varies on the history of previous surgery and the particular deformity encountered. When the plane is clearly identified, elevation of the mucoperichondrium proceeds quickly, with an appropriate length nasal speculum providing retraction onto the mucoperichondrium as well as visualization of the area where the mucoperichondrium is still attached to the septum ( Fig. 45.6 ).
With adequate vasoconstriction, anesthesia, hypotension, and dissection in the correct plane below the perichondrium, bleeding is usually not a significant problem and blood loss is minimal. A Cottle dissector is an excellent instrument to effect elevation of the perichondrial flap away from the septal skeleton. This technique works for the majority of the anterior septum as well as the posterior septum after the bony cartilaginous junction has been passed. The ligamentous attachments of the inferior septum to the spine and premaxilla are somewhat thick and the mucosa tenuous because it is frequently here that a deviation is present, requiring careful dissection to maintain continuity of the mucoperichondrial flap.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


