44 Complications in Rhinoplasty
Introduction
The nose has enormous functional, aesthetic, psychological, emotional, and social importance. 1 , 2 Most studies suggest that the great majority of aesthetic rhinoplasty patients benefit psychologically from the operation. 1 , 2 While rhinoplasty can be a satisfying procedure for both patient and surgeon, the literature reports an incidence of postoperative rhinoplasty complications ranging from 8–15%. 3 , 4 , 5 The rhinoplasty surgeon must take great care to minimize the incidence of both functional and cosmetic complications. Experienced surgeons consistently achieve a high level of satisfaction among their patients. Still, complications can occur despite technically well-performed surgery. All surgeons have complications.
How is a “complication” defined? In most cases with an unacceptable result, the patient and surgeon recognize it, and a corrective plan is agreed upon. At times, the surgeon may notice a relatively subtle abnormality that is amenable to correction, but the patient is not concerned by it. It should be a rare situation that the surgeon is proud of the outcome while the patient is displeased. 6
A candid discussion by the surgeon with the patient regarding the goals and expectations of surgery is an essential aspect of preoperative planning. A discussion of the potential complications is critical, so that the patient understands the small but real risks of a complication. Although most complications are relatively minor and correctable, more serious and debilitating complications do occur. All complications must be addressed with forthright recognition, close attention to the patient, and appropriately timed corrective measures.
Careful preoperative anatomical diagnosis cannot be overemphasized. A simplified algorithmic approach is offered here ( Tables 44.1 and 44.2 ), but further study is strongly recommended. 6 , 7 , 8 Careful anatomical examination and a conservative approach guided by an understanding of the postoperative changes that occur during healing are critical in minimizing or avoiding complications. Failure to recognize the precise anatomical cause of a nasal feature is a common reason for failure to effect the desired change. Failure in execution (e.g., greenstick osteotomies, dorsal irregularities) is another cause. Despite careful preoperative analysis and meticulous attention to surgical detail, and despite correctly performed surgery, less-than-ideal aesthetic and/or functional results may still occur.
Complications in rhinoplasty may be categorized as functional or aesthetic in nature; often, there are elements of both. In considering this subject, it will be helpful to organize aesthetic complications by the specific nasal subunit affected.
Problems after rhinoplasty commonly relate to issues of underresection, overresection, and/or asymmetry. In general, it is easier to address a problem relating to underresection, because the surgeon needs only to “take a little more.” Problems relating to overresection can be difficult, and are often complicated by scarring, need for graft material, and other issues. 3 , 6
Anatomical diagnosis is helpful in the avoidance of complications, and it is also critical in the proper evaluation and treatment of complications when they occur. This chapter addresses many of the more commonly described surgical complications with special attention to their cause and treatment. Emphasis is placed on the anatomical basis of each complication, as this approach provides a guide to correction. Although complications have been generally arranged by anatomical location, there are naturally some topics that cross categories.
By making careful study of problems encountered in a revision practice, the student of rhinoplasty can improve his or her ability to address problems encountered in both the primary and revision rhinoplasty patient, and can minimize the incidence of these problems within his or her own practice. For additional study, we would refer you to the free website www.RhinoplastyArchive.com which contains over 60 chapters and over 100 videos of rhinoplasty and revision rhinoplasty and is one of many useful resources for the lifelong learning process in rhinoplasty. 7
For the purposes of this chapter, the senior author (D.G.B.) has selected specific problems for extended discussion, either because they are problems encountered frequently, or because they illustrate specific topics or surgical techniques that may be particularly useful to the surgeon. Due to space limitations, this is by no means a complete discussion, and additional study is strongly recommended. Still, the authors hope that this information will be useful to the reader.
Nasal Tip
General Considerations
In the nasal tip, overreduction may violate critical tip support mechanisms ( Table 44.3 ), 6 , 7 , 8 , 9 , 10 which can lead to complications including tip ptosis and inadequate tip projection (see below). Alternatively, overresection of the caudal septum can result in overrotation of the nasal tip with excessive shortening of the nose. Overresection may also contribute to other complications such as bossae, alar retraction, and alar collapse. 3 , 6 , 7 , 8 , 9 , 10 , 11
Major tip support mechanisms |
1. Size, shape, and strength of lower lateral cartilages |
2. Medial crural footplate attachment to caudal septum |
3. Attachment of caudal border of upper lateral cartilages to cephalic border of lower lateral cartilages |
(Nasal septum is also considered a major support mechanism of the nose.) |
Minor tip support mechanisms |
1. Ligamentous sling spanning the domes of the lower lateral cartilages (i.e., interdomal ligament) |
2. Cartilaginous dorsal septum |
3. Sesamoid complex of lower lateral cartilages |
4. Attachment of lower lateral cartilages to overlying skin–soft tissue envelope |
5. Nasal spine |
6. Membranous septum |
Underreduction may be simply due to overcaution but is commonly due to a failure to correctly assess preoperatively the anatomical situation. For example, failure to recognize an overprojected nose, or to diagnose the steps required based on the patient’s anatomy to adequately address this, can lead to a persistent overprojected state. 9 , 12 Failure to adequately resect cartilaginous dorsum may result in a pollybeak deformity. 3 , 9 , 10 , 11 , 12 , 13
Asymmetries of the nasal tip may be due to unequal reduction of the lower lateral cartilages, or from asymmetric application of dome-binding sutures. 9 It may also be caused by unequal scarring that can occur during the natural healing process and may not be evident for months or even years after surgery. Asymmetry is often present preoperatively and should be recognized and pointed out to the patient prior to surgery.
Specific Complications in the Nasal Tip
Ptotic Tip
A critical principle in avoiding undesired changes of the nasolabial angle is assessment of tip anatomy and tip support, followed by maneuvers that maintain or augment tip support and restore the nose to a more natural appearance. As mentioned above, however, maneuvers that result in loss of tip support may lead to a droopy tip (tip ptosis with an overly acute nasolabial angle). The normal nasolabial angle (angle defined by columellar point-to-subnasale line intercepting with subnasale-to-labrale superius line) is 90–120 degrees. 14 Within this range, a more obtuse angle is more favorable in females, a more acute angle in males. Loss of tip support can lead to a ptotic, underprojected, drooping nose.
Treatment of complications relating to a ptotic nose relies on restoration of tip support and tip projection. When faced with an operative complication such as a droopy, ptotic tip, appropriate diagnosis will guide correction. 6 , 9 , 10 There are numerous rhinoplasty maneuvers to increase tip support, re-project the nose, and rotate the nose ( Table 44.4 ). 8
Increase rotation Lateral crural steal Transdomal suture that recruits lateral crura medially Base-up resection of caudal septum (variable effect) Cephalic resection (variable effect) Lateral crural overlay Columellar strut (variable effect) Plumping grafts (variable effect) Illusions of rotation—increased double break, plumping grafts (blunting nasolabial angle) |
Decrease rotation (counter-rotate) Full transfixion incision Double layer tip graft Shorten medial crura Caudal extension graft Reconstruct L-strut, as in rib graft reconstruction (integrated dorsal graft/columellar strut) of saddle nose |
Increase projection Lateral crural steal (increased projection, increased rotation) Tip graft Plumping grafts Premaxillary graft Septocolumellar sutures (buried) Columellar strut (variable effect) Caudal extension graft |
Decrease projection High partial, or full transfixion incision Lateral crural overlay (decreased projection, increased rotation) Nasal spine reduction Vertical dome division with excision of excess medial crura, with suture reattachment |
Increase length Caudal extension graft Radix graft Double layer tip graft Reconstruct L-strut |
Decrease length See increase rotation Also, deepen nasofrontal angle |
Overrotated Tip
Conversely, one may face a patient with a nose that has been overrotated, with an overly obtuse angle. Overresection of the caudal septum is a common cause of overrotation of the tip. Overrotation of the nose creates an unsightly, overshortened appearance.
Careful preoperative assessment can identify those patients in whom operative rotation should be avoided. Treatment of complications relating to a short, overrotated nose rely on maneuvers that lengthen and counterrotate the nose. 9 , 10 There are specific rhinoplasty maneuvers to lengthen and counterrotate the nose ( Table 44.4 ). 8
Bossae
A bossae is a knuckling of the lower lateral cartilage at the nasal tip due to contractural healing forces acting on weakened cartilages. Patients with thin skin, strong cartilages, and nasal tip bifidity are especially at risk. Excessive resection of lateral crus and failure to eliminate excessive interdomal width may play some role in bossae formation. Bossae are felt to be the result of scar contracture on an overly narrowed complete rim strip, causing a bulging during postoperative healing. Some have described an association between cartilage splitting techniques and bossa formation. 3 Others, however, maintain that vertical dome division techniques are reliable when performed correctly and do not contribute to these difficulties. 11 , 15
As an isolated deformity, bossae are typically treated through a small marginal incision with minimal undermining over the offending site followed by trimming or excising the offending cartilage. In some cases, the area is covered with a thin wafer of cartilage, fascia, or other material to further smooth and mask the area.
Alar Retraction/Alar–Columellar Disproportion
Cephalic resection of the lateral crus of the lower lateral cartilages is commonly undertaken to effect refinement of the nasal tip. If inadequate cartilage is left, then the contractile forces of healing over time will cause the ala to retract ( Fig. 44.1 ). 3 , 9 , 10 , 11 , 16

This is a commonly seen sequelae of overresection of the lateral crus. The surgical rule-of-thumb is to preserve at least 6–9 mm of complete strip. Nevertheless, an anatomical study of the alar base recognized that in a normal patient population, 20% of patients had a thin alar rim. This anatomical variation must be recognized, as these patients may require even more conservative approaches to avoid the risk of alar retraction and/or external nasal valve collapse. 17 Also, vestibular mucosa should be preserved, as excision of vestibular mucosa contributes to scar contracture with alar retraction.
Alar retraction may be treated by cartilage grafts in more minor cases (1–2 mm). 3 The area of retraction is marked prior to injection, and a small marginal incision allows dissection of a precise pocket. A contoured cartilage graft (commonly of auricular or septal cartilage) may be inserted into the precise pocket, which should extend inferiorly to the sesamoids and should be wide enough to simulate the normal shape of the lateral crus at the dome.
Auricular composite grafts are commonly used in more severe cases. The cymba concha of the opposite ear (e.g., left ala, right ear) provides the best contour. An incision several millimeters from the nostril rim is followed by careful dissection with freeing of adhesions, creating a defect and displacing the alar rim inferiorly. The fashioned composite graft is carefully sutured into place. 3 , 18
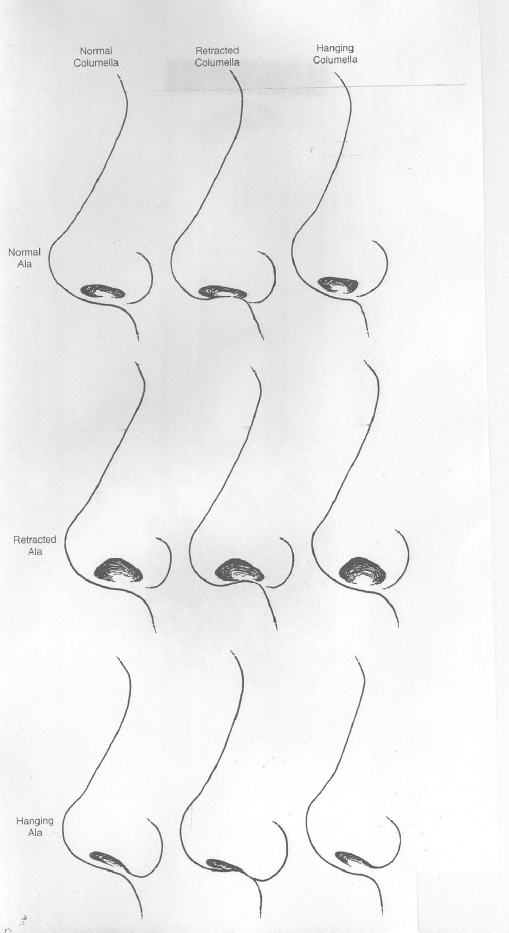
Alar–columellar disproportions (protruding or hanging columella) can be areas of significant patient concern. 19 , 20 The range of normal columellar show is generally considered to be 2–4 mm. The complexities of the alar–columellar relationship have been categorized by Gunter, 20 who describes the position of the ala and the columella in relationship to a line drawn through the long axis of the nostril. 20 All patients have a hanging, normal, or retracted ala and a hanging, normal, or retracted columella. Thus, there are nine possible anatomical combinations making up the alar–columellar relationship ( Fig. 44.2 ).
Alar–columellar disproportion may exist in the unoperated nose; also, it may be caused by surgical misadventure ( Fig. 44.1 ). A protruding or hanging columella may be due to a persisting uncorrected deformity, such as overly wide medial crura or overlong caudal septum. 9 The deformity may be increased columellar show secondary to retraction of the alar margins, rather than an actual protrusion of columella. A deficient or retracted columella may be due to a preexisting uncorrected deformity, or it may be due to excessive resection of soft tissue, cartilage, or nasal spine. The surgeon should avoid excessive resection of the caudal septum, and should avoid resection of the nasal spine. 3 , 9 , 19
Treatment of a protruding or hanging columella may include retrodisplacing the medial crura onto the caudal septum in a tonguein-groove fashion. At times, resecting fullthickness tissue from the membranous columella, including skin, soft tissue, and perhaps a portion of the caudal end of the septum itself, may be indicated. If the medial crura is excessively wide, excision may include a conservative excision of the caudal margin of the medial crura. 9 , 19
Retracted columella may be improved with plumping grafts inserted at the base of the columella to address an acute nasolabial angle; columellar struts may also be helpful for minor deformities. A cartilage graft may be used to lengthen the over-shortened nose. The use of composite grafts has also been described. 3 , 9
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


