42 Percutaneous/Kapandji Pinning
Abstract
Closed reduction and percutaneous pinning of a distal radius fracture is a surgical option when closed manipulation and splinting have failed to provide adequate fracture reduction. Fractures best suited for this technique include extra-articular fractures without significant comminution in patients with adequate bone stock. Pinning can be performed in a standard fashion across the fracture site or using the intrafocal (Kapandji) method, where the pins are inserted into the fracture site, used to maneuver the fracture alignment, and then driven into the far (usually the volar) cortex to maintain the position of the fracture. The main bailout of this procedure is open reduction and internal fixation (ORIF) with plates and screws in cases where either reduction cannot be achieved by closed means or if the fixation construct is deemed to be unstable.
42.1 Key Principles
Careful analysis of the fracture pattern and a thorough understanding of fracture biomechanics are a prerequisite to successful utilization of this minimally invasive technique. Awareness of the limitations of this technique allows the surgeon to prevent failures and the need to resort to bailout procedures such as external fixation open reduction and internal fixation (ORIF) with plates and screws or bridge plating.
42.2 Expectations
Articular congruency at the radiocarpal and distal radioulnar joint (DRUJ) must be established, and volar tilt, radial height, and inclination must be restored. Stability of DRUJ should be assessed once the distal radius is pinned. Instability may indicate the need for soft tissue repair and/or pinning of DRUJ.
42.3 Indications
Percutaneous techniques are most successful in the acute period, within the first 2 to 3 weeks postinjury due to limited callus formation and relative mobility of the fracture fragments. This technique is indicated in fractures that can be reduced by traction, manipulation, and ligamentotaxis. This approach can be considered primarily in patients with dorsally displaced, extraarticular fractures with minimal comminution. Patients with intra-articular fractures that are minimally comminuted such as radial styloid fractures can also be treated with this technique. The ideal patients indicated for this technique are younger with good bone stock.
42.4 Contraindications
Shear fractures, the presence of severe intra-articular or metaphyseal comminution, and poor bone stock usually preclude the use of the percutaneous technique. Bilateral fractures are a relative contraindication due to issues with hygiene and performance of activities of daily living.
42.5 Special Considerations
A detailed preoperative radiographic assessment is necessary to identify the appropriate candidate for this procedure. The patient’s comorbidities, age, and the age of the fracture aid in decision making. A major advantage of this technique is its low cost and minimal instrumentation needs.
42.6 Special Instructions, Positioning, and Anesthesia
Upper arm tourniquet
Brachial plexus block usually adequate
10 to 15 lbs of traction can be helpful via finger traps on index and middle fingers
Intraoperative fluoroscopy (mini C-arm)
Instrumentation necessary if there is a need to convert to ORIF or external fixation and/or use of dorsal spanning plate
42.7 Tips, Pearls, and Lessons Learned
42.7.1 To Incise or Not to Incise Skin
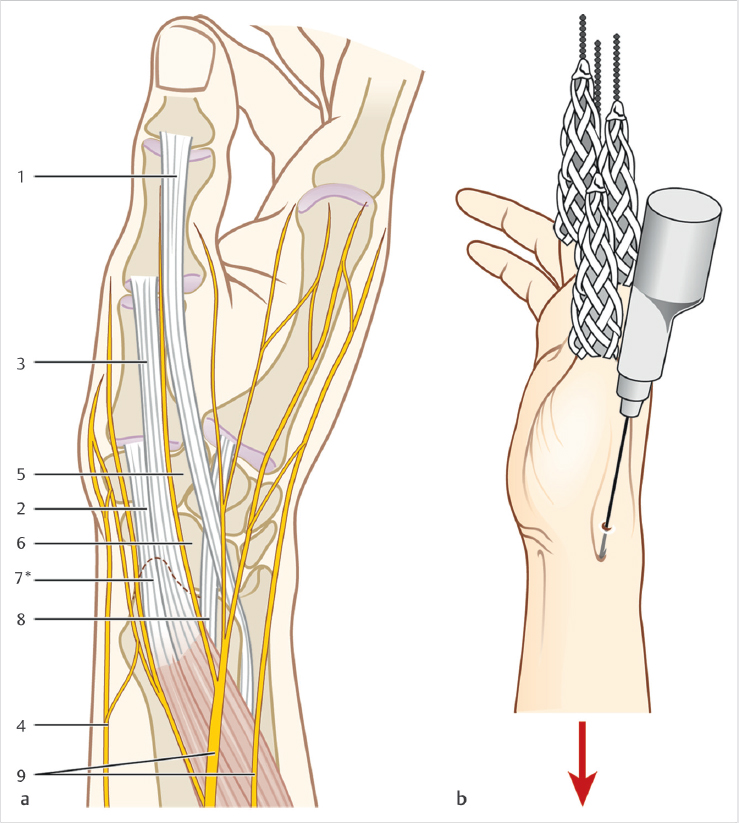
Injury to the superficial radial nerve or extensor tendons is possible. Some surgeons prefer to make 1to 1.5-cm incisions and to use soft tissue guides for the safe placement of Kirschner wires (K-wires) about the distal radius (► Fig. 42.1).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


