43 Distal Radius: Volar Approach
Abstract
The volar approach for fixation of distal radius fractures has become more popular in the past years due to the introduction of locking metal plates and screws specifically designed to match the distal radius topography. In addition, other benefits include a decreased rate of tendon-related complications such as irritation and rupture. The traditional Henry approach is commonly used, but other approaches such as the trans–flexor carpi radialis approach and the volar extensile approach that includes the carpal tunnel release are also used.
43.1 Description
There are different intervals through which the radius can be approached from the volar aspect. The best known is the classical Henry approach, while others include the trans-flexor carpi radialis (FCR) approach and the volar extensile approach (including a carpal tunnel release). Other modifications have been added including the two-windows approach 1 or the mini-open approach. 2
43.2 Key Principles
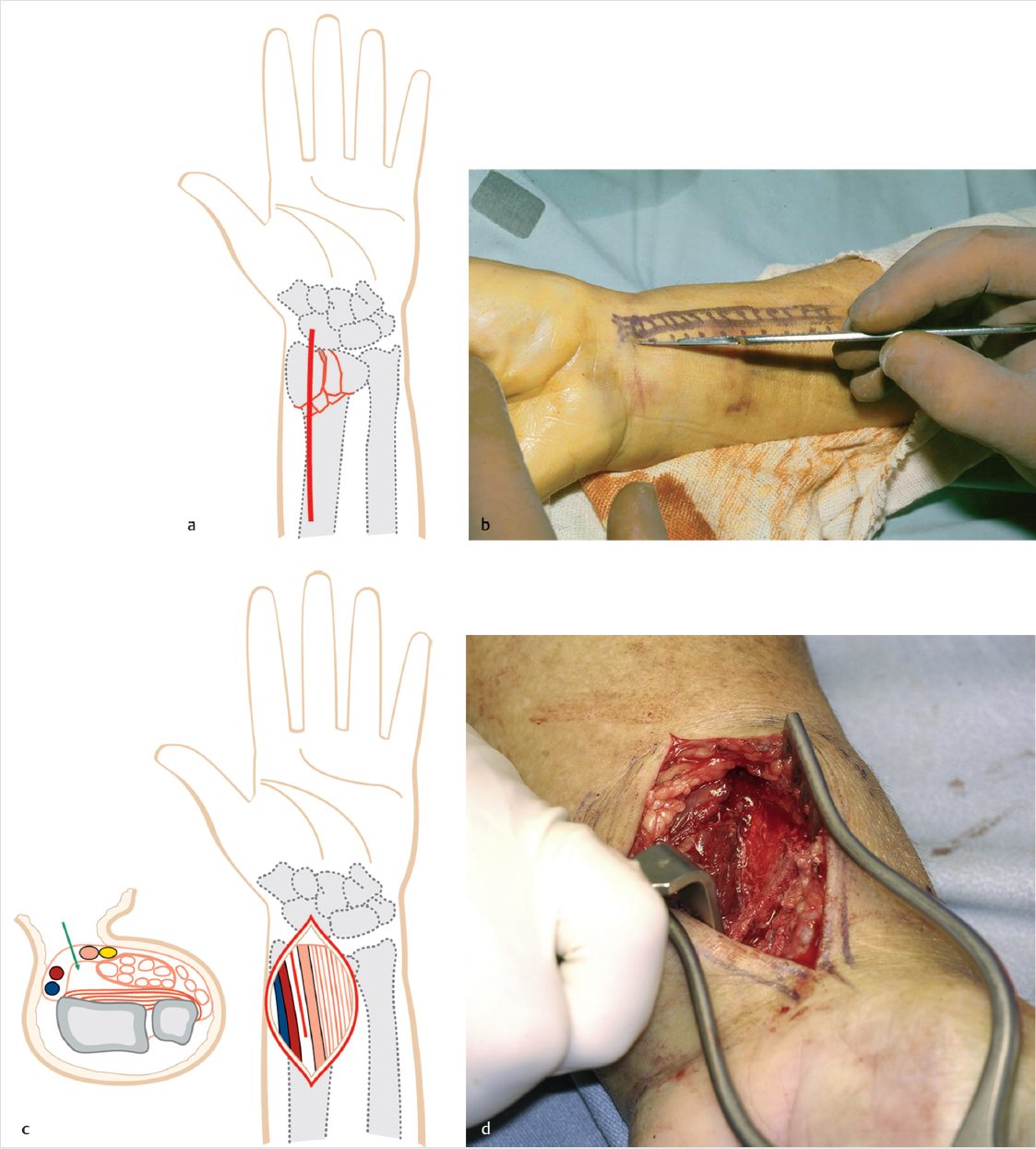
A thorough knowledge of the wrist and forearm anatomy is essential. The superficial anatomical landmarks are the FCR tendon, the radial artery, the palmaris longus (PL) tendon, and the flexor carpi ulnaris (FCU) tendon. The location of the median nerve (including the palmar cutaneous branch), the flexor pollicis longus (FPL) tendon, and the pronator quadratus (PQ) are also important.
43.3 Advantages
The volar approach has become more popular in the past years due to the introduction of locking metal plates and screws specifically designed to match the topography of the distal radius. In addition, other benefits include a decreased rate of tendonrelated complications such as irritation and rupture, and the biomechanical advantage of placing the plate on the tensile side. 3
43.4 Indications
Most of the distal radius fractures that require surgical treatment could be addressed from a volar approach, such as unstable intraor extra-articular fractures with either a dorsal apex or a volar apex pattern, or partial articular fracture that requires fragment-specific fixation.
43.5 Contraindications
Contraindications include dorsal shear fractures that may be better treated from a dorsal approach, fractures that require double approach, and open fractures with inadequate soft tissue. In addition, fractures with severe comminution or complex articular surface disruption may better be treated with a bridge plate or an external fixator.
43.6 Considerations
Previous identification of the fracture pattern by radiological images will allow a preoperative planning of the approach needed.
43.7 Requirements, Positioning, and Anesthesia
A radiolucent hand surgery table, tourniquet, and fluoroscopy (mini C-arm) are needed
Forearm in supine position
Anesthesia can be general or via a regional nerve block
43.8 Approach
43.8.1 Henry Approach
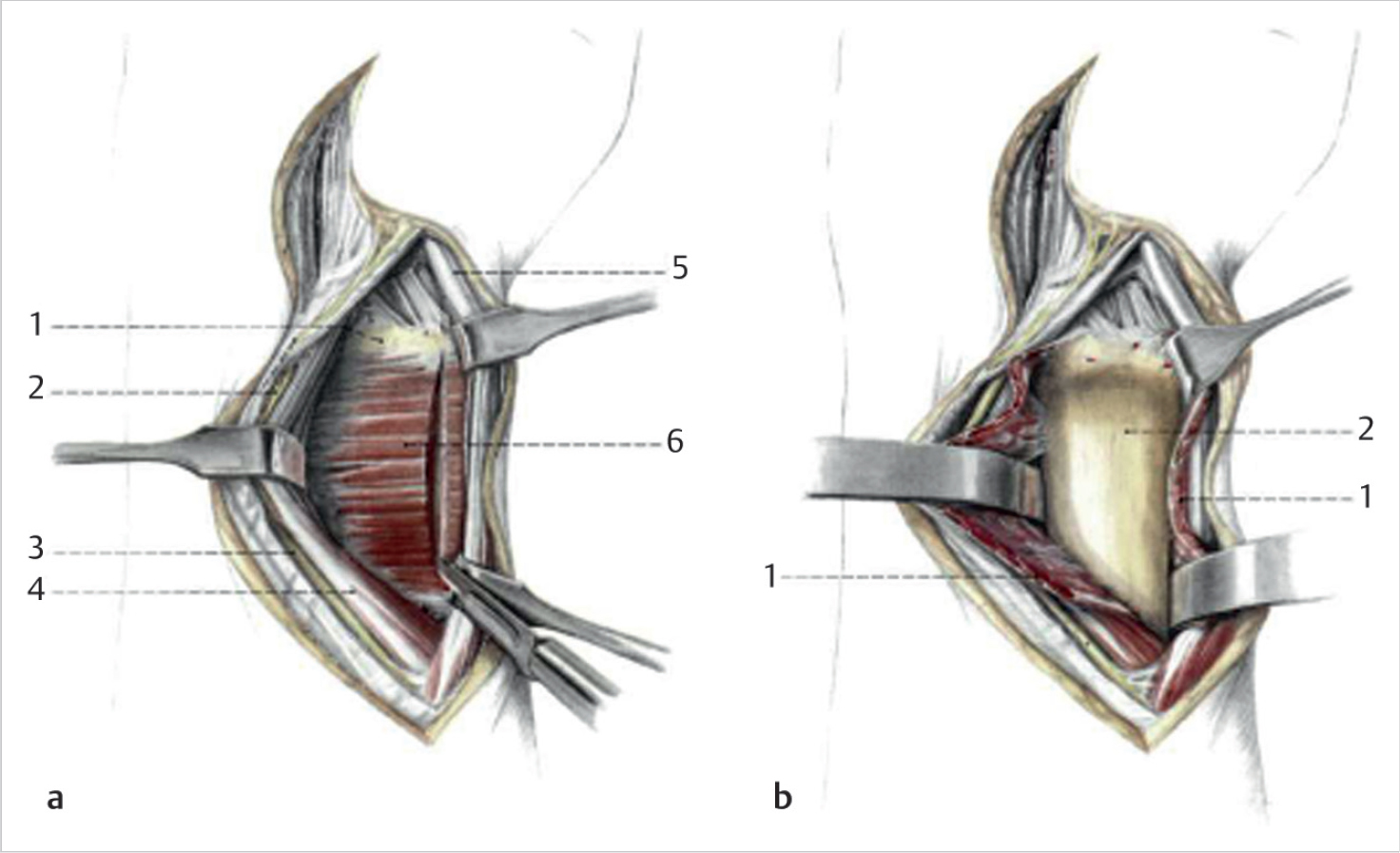
An incision is made between the radial artery and the FCR tendon, and the interval explored (► Fig. 43.1). The superficial forearm fascia is incised and the contents of the volar forearm retracted. The PQ is released from the distal and radial insertion to expose the fracture (► Fig. 43.2). 4
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


