44 Dorsal Approach to Distal Radius
Abstract
Volar approach is commonly used for fixation of distal radius fractures. There are certain fracture patterns for which dorsal approach is recommended. This chapter outlines the indications for dorsal approach to distal radius fractures.
44.1 Introduction
Distal radius fracture is one of the most common injuries to the musculoskeletal system. There are multiple treatment options ranging from nonoperative management, closed reduction and pinning, and closed reduction and external-fixator application to open reduction internal fixation. Open reduction and volar plate fixation has become the preferred treatment for most of these fractures. 1 However, there are several fracture types for which dorsal approach is more suitable. This chapter outlines the indications for dorsal approach to distal radius fractures along with case examples.
44.2 Indications
Dorsal approach to distal radius is indicated for the following:
Radiocarpal fracture dislocation.
Dorsal shearing fracture of the lunate facet.
Displaced and irreducible dorsal-ulnar (die-punch) fragment.
Irreducible dorsal articular impaction and articular surface reconstruction.
Associated scaphoid fracture.
Associated carpal ligament injury.
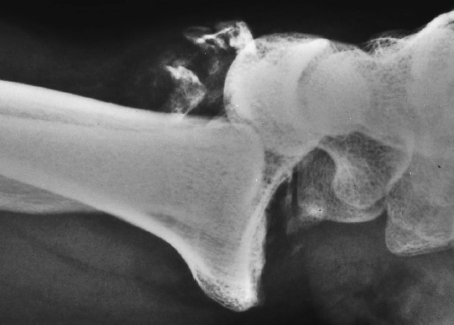
Radiocarpal fracture-dislocations are complex injuries characterized by dislocation of the radiocarpal joint (► Fig. 44.1). It is important to differentiate these from a Barton or reverse Barton (dorsal) fracture (► Fig. 44.2). Barton’s fracture involves a shear fracture of the articular surface of distal radius, with the fractured fragment attached to the carpus. In addition, the displaced fragment forms a substantial part of the distal radius articular surface. In contrast, radiocarpal fracture-dislocation is a high-energy injury with disruption of the radiocarpal ligaments. It is typically associated with a small cortical rim and/or radial styloid fracture (► Fig. 44.1).

Dumontier et al 2 proposed a classification system for radiocarpal dislocations. Type 1 is very rare and concerns primarily ligamentous injuries. Type 2 radiocarpal dislocations are associated with fractures of the radial styloid that involves more than 1/3rd of the width of scaphoid fossa and may continue to the dorsal margin of distal radius. The authors recommended repair of the volar ligamentous structures for type 1 injuries and a dorsal approach with fixation of the radial styloid fragment for type 2 injuries.
Calderon et al 3 described 20 patients with dorsal shear fractures associated with radiocarpal subluxation or dislocation. The authors found that these fractures involved dorsal shear fragments associated with (a) central impaction; (b) impaction of majority of distal radius articular surface; and (c) radiocarpal dislocations with rupture of the radiolunate ligaments or fracture of the volar portion of the lunate facet, where radiolunate ligaments originate. The authors recommended the dorsal approach to buttress the dorsal shear fractures and reconstruct the articular surface for associated central impaction. A combined volar approach was recommended for volar ligamentous repair or fixation of small volar avulsion fracture in radiocarpal dislocations with dorsal shear fractures

44.3 Surgical Technique
44.3.1 Case 1
A 30 y/o male sustained a fall from a height and presented with right distal radius fracture. PA and lateral radiographs revealed a complex radiocarpal fracture-dislocation of his right wrist (► Fig. 44.3). Sagittal, two-dimensional CT views demonstrate the very small shearing fracture of the dorsal aspect of the distal radius with dislocation of the carpus (► Fig. 44.3).
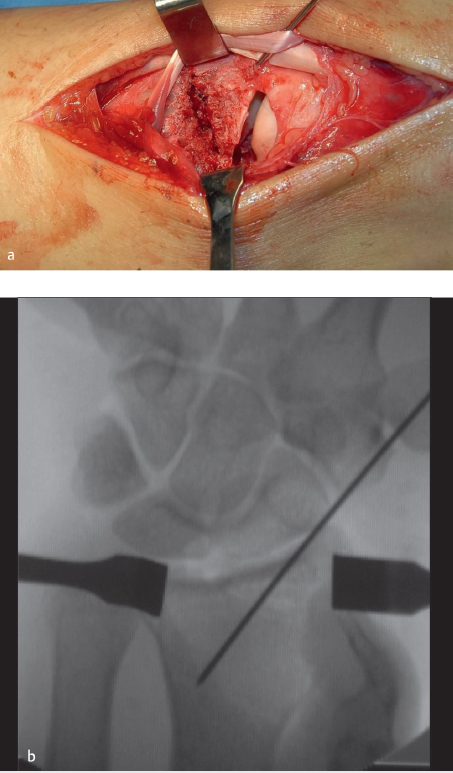
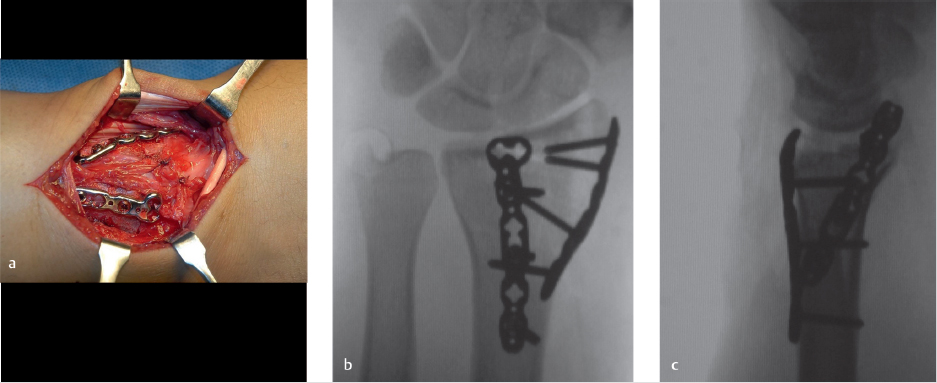
Three-dimensional CT reconstructions show the volar rim of the radius to be intact with the dorsal small shearing fracture fragments (► Fig. 44.3). Also seen in all the preoperative images is the radial styloid fracture. Notice the horizontal fracture line involving the entire scaphoid fossa and continuing to the dorsal cortical rim. Operative fixation was recommended. A standard dorsal approach to the wrist was used, with a longitudinal incision over distal radius and radiocarpal joint in line with the 3rd metacarpal. The extensor pollicis longus tendon was mobilized from the 3rd dorsal compartment and the tendons of the second and fourth dorsal compartment were retraced to gain exposure (► Fig. 44.4). The dorsal small rim and the radial styloid fractures are clearly visualized. Usually the capsule is torn (► Fig. 44.4), but if it is intact, a dorsal arthrotomy is made parallel to the dorsal rim to inspect the articular surface and look for any associated carpal injury. At this point, carpus is reduced and fixation is started with the less comminuted fracture fragment. In this case, a 0.062 smooth K-wire was used for provisional fixation of the radial styloid fracture, and articular reduction was also confirmed using intraoperative fluoroscopy (► Fig. 44.4). If dorsal rim fragments are adequately large, provisional fixation can be obtained with K-wires. If they are too small, they can be held with suture anchors or transosseous sutures. Low-profile dorsal-distal radius plates were then used for fragment-specific fixation (► Fig. 44.5). Radial column plate and 2.4 mm dorsal plate were used. Capsule was repaired using resorbable suture (► Fig. 44.5). Follow-up at 8 months showed excellent function with some loss of wrist extension and flexion (► Fig. 44.6). Many plates are available for these fractures. The most recently designed plates have variable angle locking screws. The dorsal plate should be applied as distally as possible. These plates might need some contouring to fit the distal radius metaphysis and the radial styloid.

Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


