45 Bridge Plating of Distal Radius Fractures
Abstract
There exist a variety of methods to repair distal radius fractures. A challenging subset of these fractures includes those with substantial articular comminution or significant meta-diaphyseal extension. Historically, these fractures were treated with external fixators. Another recently described option is dorsal spanning or bridge plate fixation which consists of internal distraction plating. A plate is spanned dorsally from the index or long finger metacarpal to the shaft of the radius to provide stable fixation allowing for distraction across severely impacted and comminuted distal radius fractures.
45.1 Description
The use of bridge plating for the treatment of distal radius fractures is one option in the armamentarium of surgeons for the management of a complex set of distal radius fractures with specific treatment challenges. It was first described by Burke and Singer as a stable construct and alternative to external fixators. 1
45.2 Anatomy
A thorough understanding of the relevant anatomical structures is key for the management of distal radius fractures. Restoration of wrist anatomy in order to regain function is usually associated with satisfactory outcomes.
45.2.1 Bones
The wrist is a complex joint that consists of two long bones and eight carpal bones. There are three main articulations (► Fig. 45.1):
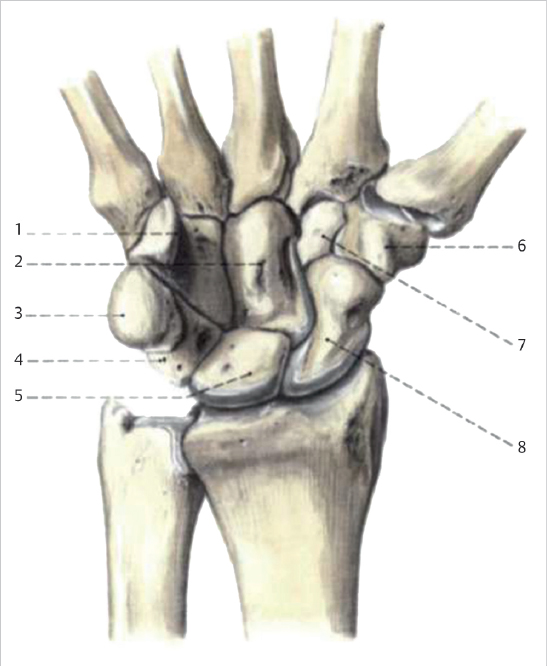
Radiocarpal: Distal radius and triangular fibrocartilage complex (TFCC) to proximal row
Distal radioulnar joint (DRUJ)
Midcarpal: Between the proximal and distal carpal bone rows
45.2.2 Biomechanics
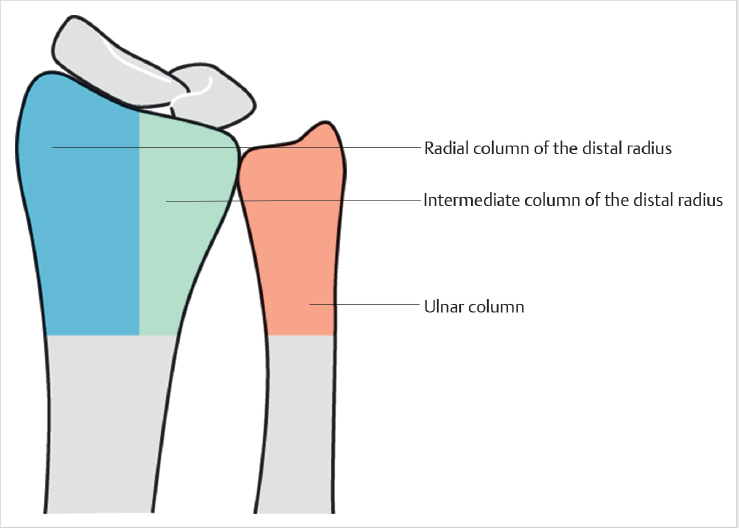
Biomechanics of the wrist joint via the Column Concept:
Radial column: Includes the radial styloid and scaphoid fossa
Intermediate column: Includes the lunate fossa and sigmoid notch
Ulnar column: Includes the distal ulna with the TFCC
The column concept proposes a theory in which load is transmitted throughout the wrist (► Fig. 45.2). Under normal physiologic conditions, the majority of load is transmitted across the intermediate column and a minor amount along the radial column. The ulnar column also withstands a significant load as it serves as the stabilizer of wrist pronation/supination, flexion/extension, and radial/ulnar deviation. 2
45.2.3 Radiographic Parameters
Melone described three standard radiographic parameters of the distal radius as follows (► Fig. 45.3) 3 :
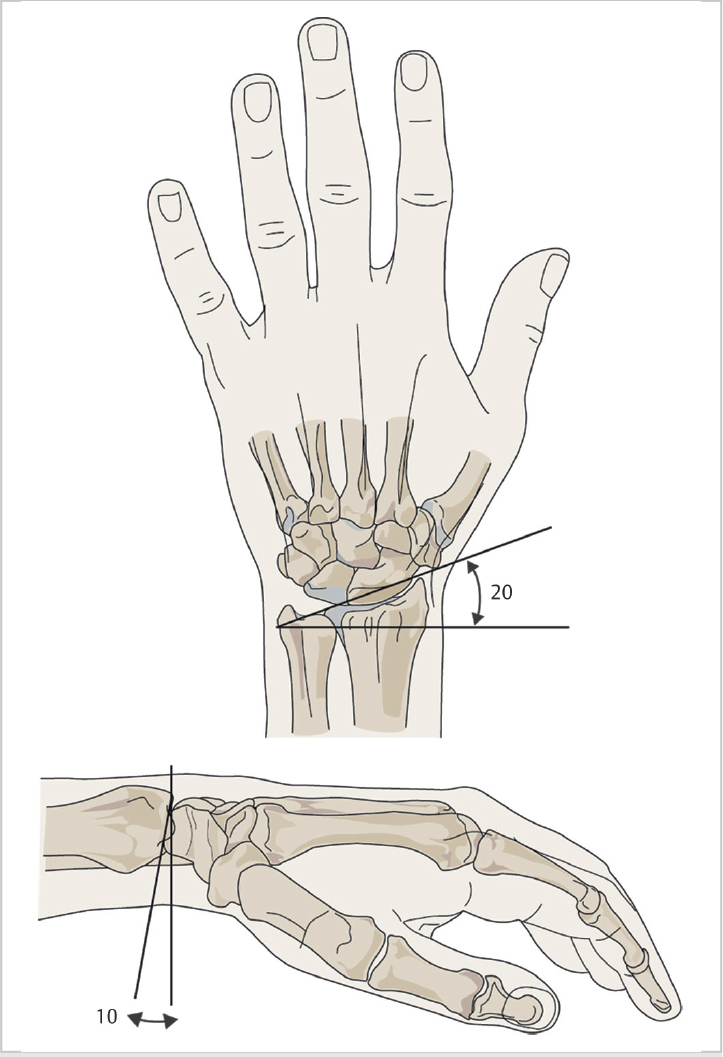
Radial inclination: The angle formed between the line drawn from the tip of the radial styloid to the ulnar corner of the distal radius articular surface with respect to the line perpendicular to the radial shaft. Average measurement is 23°.
Volar tilt: The angle formed between the line drawn perpendicular to the long axis of the radius and the line between the dorsal and volar lips of the distal radial articular surface. Average measurement is 11°.
Radial height: The distance measured between the two parallel lines drawn perpendicular to the long axis of the radial shaft. One is drawn from the tip of the radial styloid and the other from the ulnar corner of the lunate fossa. Average measurement is 11 to 12 mm.
45.2.4 Extensor Compartments
With bridge plating, an apparatus intimately involving the extensor compartments is utilized (► Fig. 45.4). These compartments are as follows:
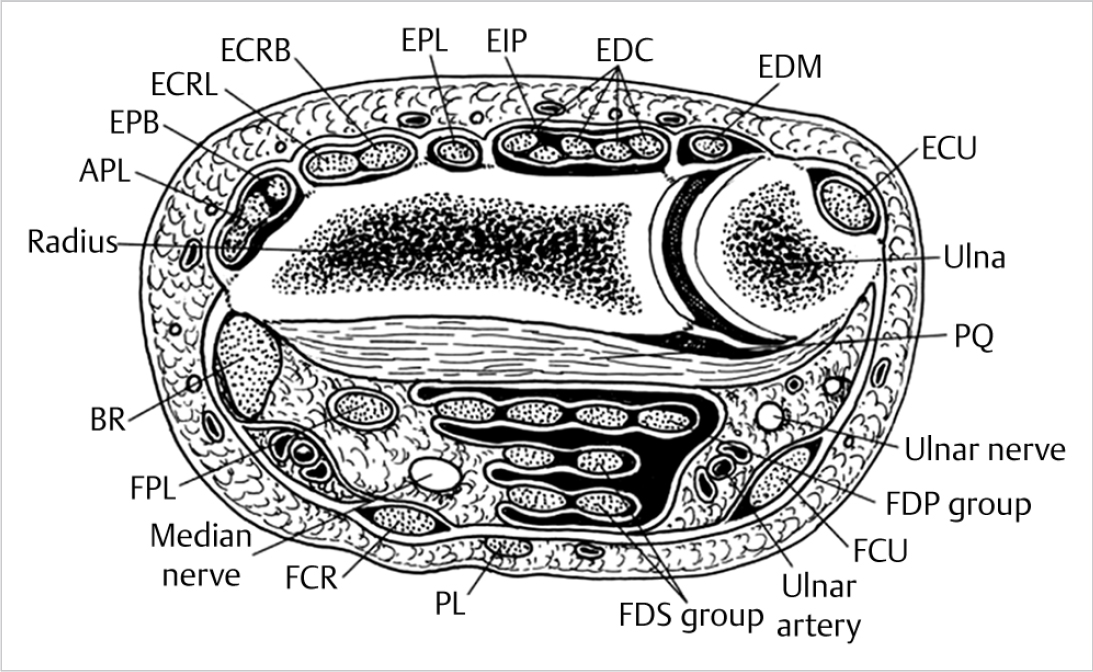
Abductor pollicis longus (APL) and Extensor Pollicis brevis (EPB)
Extensor carpi radialis longus (ECRL) and Extensor carpi radialis brevis (ECRB)
Extensor pollicis longus (EPL)
Extensor indicis propius (EIP) and Extensor digitorum communis (EDC)
Extensor digiti minimi (EDM)
Extensor carpi ulnaris (ECU)
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


