4 Techniques for Office Anesthesia: Local Anesthesia and Regional Block Techniques
Key Concepts
Local anesthetics in regional nerve blocks provide analgesia by blocking pain transmission along specific nerve fibers.
The target of local anesthetics is the sodium channel.
The degree of nerve blockage depends on the particular local anesthetic drug used and its concentration and volume.
Knowledge of reliable anatomic bony and muscular landmarks is the key to precise local anesthetic placement.
Detailed description of anatomy and techniques of regional blocks of the face, neck, and anterior chest are reviewed in this chapter.
The secret to achieving full-face analgesia via local anesthetics is familiarity with the important but less universally known blocks of the external nasal, anterior ethmoid, lacrimal, buccal, zygomaticotemporal, and auriculotemporal nerves.
Systemic toxicity from clinical dosages of local anesthetics is a potential but uncommon event.
Cardiotoxicity is more frequent with high-potency, lipid-soluble agents such as bupivacaine and ropivacaine.
Introduction
A growing demand for cosmetic procedures outside the operating room has driven the need for physicians skilled in the practice of local anesthesia. The delivery of local anesthetic care is a blend of artistry and science. The ability to safely and effectively apply these techniques can make all the difference in creating good surgical results as well as pleased and satisfied patients. The use of local anesthetics in an office setting ranges from topical application, local infiltration, and field blocks to, importantly, regional blocks. The key to successful regional anesthesia relies heavily on detailed knowledge of local anatomy; and nowhere else is this as demanding as in the head and neck. Proper application of local anesthetics plays a critical role in procedures ranging from repair of lacerations to lesion-directed biopsies and full-face ablative laser resurfacing.
The advantages of local, compared with general, anesthesia are many. First, the airway is not compromised; therefore, the patient can control breathing, eliminating the risk of respiratory depression and all its untoward consequences. Second, a patient who is awake is also able to aid in positioning. This assists in surgical maneuvers like assessment of upper eyelid skin excision in blepharoplasty to ensure appropriate lagophthalmos. Third, the immediate postoperative recovery is smoother, without the coughing or bucking seen with extubation. Fourth, there is better postoperative pain control because the local anesthetic wears off slowly. Fifth, bleeding is less, due to the vasconstrictive properties of concomitant epinephrine and lack of vasodilatory effects of inhalation agents. Sixth, early discharge is possible because patients do not experience a depressed level of consciousness. Last, costs are reduced because operating-room fees and hospital stays can be avoided.
The disadvantages of using only local anesthesia are many, as well. First, some patients are fearful of undergoing surgery while awake. Second, local anesthetics have systemic side effects that can reach toxic levels. Third, techniques for injecting local anesthetics are learned, thus poor injection skill may result in inadequate anesthesia and unnecessary pain. Fourth, the effects of local anesthesia are not immediate—particularly in the case of nerve blocks—so proper planning and time management need to be factored into the procedure to ensure optimal patient comfort. Fifth, if intraneural injection occurs, there is a very small risk of permanent nerve damage. Last, local anesthetics have decreased potency in an acidic environment such as an infected area.
Background: Basic Science of Procedure
Cocaine, an extract of the coca leaf, was the first successful local anesthetic.1 Although Sigmund Freud published extensively on cocaine and its effects, the recognition for the discovery of local anesthesia belongs to Karl Köller, a friend and colleague of Freud. In 1884, with the application of cocaine to the conjunctiva and cornea of animals, Köller introduced the first use of local anesthetic in surgery.2–4 By 1892, the use of cocaine in peripheral nerve blocks had been launched by W.S. Halsted, professor of surgery at Johns Hopkins University and later the creator of the residency system in surgery.3
Local anesthetics are classified biochemically into two groups: amides and esters. Structurally, each consists of an aromatic benzene ring joined to an amino group with either an ester or an amide linkage. Of note, the amide link is less heat-labile and therefore more stable in settings of pH or temperature fluctuations. Both groups are also categorized as weak bases, and thus can exist in one of two forms—a lipid-soluble neutral form or a charged hydrophilic form. The neutral form is understood to contribute to penetration of the drug into the neural cytoplasm; whereas the charged form is the active structure that interacts with the sodium channels.
Local anesthetic agents act by targeting the sodium channel. This sodium channel blockade results in an attenuation of neural action potential formation and propagation. Studies reveal that a 50% loss in action potential must be achieved before clinical loss of function is evident.5 After application of local anesthetics to a peripheral nerve, the first sense to be blocked is temperature, followed by sharp pain, and then light touch.
Systemic absorption of local anesthetics is governed by several factors. The anesthetic′s pharmacokinetic properties, dose, site of injection, and the addition of a vasoconstrictive agent all influence the rate of absorption. The rate of absorption differs among individual local anesthetics. More lipid-soluble anesthetics demonstrate slower rates of absorption. Local anesthetics are known to vasoconstrict vessels at low doses but in concentrations used for clinical practice actually vasodilate via direct action on smooth muscles of vessel walls. The only exception to this rule is cocaine, which consistently produces vasoconstriction.4 In vessel-rich areas, higher peak plasma levels can be achieved in a short period of time unless concomitant vasoconstrictors are utilized. The greatest rate of systemic absorption is seen with intercostal nerve blocks, as compared with other sites in the body.5 Use of vasoconstricting agents—the most popular, epinephrine—clinically results in longer duration of anesthesia, decreased risk of toxic side effects, and reduced bleeding in the surgical field. In a 70 kg healthy individual, the toxic dose of 1% lidocaine with 1:100,000 epinephrine is 50 mL or 7 mg/kg.
Clearance of local anesthetics is determined by their chemical linkage. Amino esters are hydrolyzed by plasma cholinesterases, whereas amino amides are degraded hepatically by carboxylesterases and cytochrome P450 enzymes. Therefore, cardiac and hepatic disease states may alter pharmacokinetics, and lower dosages of local anesthetics should be indicated. Renal disease, alternatively, has very little effect on the pharmacokinetics of local anesthetics.
The choice of local anesthetic depends on the length of procedure or surgery and preference for postoperative analgesia ( Table 4.1 ). Esters include cocaine (Lannett Company Inc., Philadelphia, PA), procaine (Hospira, Inc., Lake Forest, IL), and tetracaine (Alcon Laboratories, Inc., Ft. Worth, TX). Commonly used amides are lidocaine (APP Pharmaceuticals, LLC, Schaumberg, IL), prilocaine (Dentsply Pharmaceuticals, York, PA), mepivacaine (Hospira, Inc., Lake Forest, IL), bupivacaine (Hospira, Inc., Lake Forest, IL), and ropivacaine (Naropin, APP Pharmaceuticals, Schaunberg, IL).
Patient Selection
A frank discussion needs to take place to reconcile both patient expectations and procedure-specific factors, when performing procedures under only local anesthetic. Patient factors such as psychological reserve, pain tolerance, anxiety, stamina, and tolerance must be thoroughly evaluated. Because the patient will be awake throughout the procedure, the physician needs to be candid in terms of the intensity of stimulation anticipated and the duration of the operation. Often these procedure-specific factors depend considerably on the skill of the physician as well. The operative team also needs to be sensitive with respect to conversation, music, and sudden noises during the surgery. If any of these points pose a concern to either the patient or physician, further sedation options, ranging from light or “conscious” sedation to general anesthesia, can be explored ( Table 4.2 ). In our clinical practice, for surgeries requiring full-face regional blocks, we routinely utilize “conscious” sedation (ASA [American Society of Anesthesiologists] category I and II patients) with Versed (Roche Laboratories, Nutley, NJ) and fentanyl titrated to help mitigate the discomfort of multiple regional blocks. This is not absolutely necessary; however, we find that most patients prefer this combination to ensure a pleasant process.
Agent | Onset (min) | Peak (min) | Duration (min, h) |
Esters | |||
Cocaine | Immediate | – | 45 min |
Procaine | 2–5 | <15 | 60 min |
Tetracaine | 2–8 | – | 4–5 h |
Amides | |||
Lidocaine | 3–5 | – | 1–2 h |
Bupivacaine | 2–10 | 30 | 3–6 h |
Ropivacaine | 1–15 | 20–45 | 5–8 h |
Abbreviations: min, minutes; h, hours. | |||
1 | No sedation or analgesia |
2 | Light sedation and/or analgesia—“conscious” sedation |
3 | Moderate sedation and/or analgesia |
4 | Deep sedation |
5 | General anesthesia |
True allergic reactions to local anesthetics are very rare. Antigenicity, mediated either through a type I (IgE) or type IV (cellular immunity) reaction toward local anesthetics, is often related to the presence of its ester or amide linkage. It is known that esters are more likely to cause an allergic reaction. Reports of true type I allergic reactions are purported to be a result of the ester′s hydrolysis into its para- aminobenzoic acid constituent, which is a documented allergen.5 Alternatively, allergic reactions may be a result of added preservatives, such as methylparaben or metabisulfite.
Frequently, clinical history points toward intolerance of the epinephrine within the local anesthetic, as opposed to a true allergic reaction. Epinephrine is a sympathomimetic amine and both an α- and β-adrenergic stimulant. It is an excellent vasoconstrictor with potential systemic side effects. Epinephrine has been shown to increase heart rate, stroke volume, cardiac output, and oxygen consumption in the cardiovascular system. Further, it may act as an irritant to the myocardium, predisposing to premature ventricular contractions and other dysrhythmias. Epinephrine should be limited to 0.04 mg in patients with a cardiac history. Most local anesthetics include 1:100,000 epinephrine, which is equivalent to 0.01 mg/mL ( Table 4.3 ).6 This agent is contraindicated in patients to whom β-adrenergic stimulation is harmful, and who present with unstable angina, malignant arrhythmias, and uncontrolled hypertension.7 Anyone taking medications that alter the effects of catecholamines—such as tricyclic antidepressants or monoamine oxidase inhibitors (MAOIs)—should also avoid epinephrine.
Agent | Concentration | Dosage |
Lidocaine | 0.5% | 5 mg/mL |
1% | 10 mg/mL | |
2% | 20 mg/mL | |
Epinephrine | 1:100,000 | 10 µg/mL |
1:200,000 | 5 µg/mL | |
1:1,000 | 1,000 µg/mL | |
Cocaine | 4% | 40 mg/mL |
Technical Aspects of Procedure
Topical Anesthetics
Local anesthetics are also commercially available in topical preparations for both the skin and mucous membranes. Although topical agents are not injected, one must still be mindful of potential systemic toxicity because a high degree of permeability is seen with topical application. For the oral mucosa, 10% aerosol lidocaine or 4% viscous lidocaine is an effective agent. For the conjunctiva and cornea of the eyes, 4% ophthalmic tetracaine is an ideal option. The vasoconstrictive properties of 4% cocaine make it a favorite among rhinologic surgeons. However, cocaine also acts as a mucosal irritant in chronic abuse, making it the culprit in septal perforations. Medical indications for cocaine use are scrutinized not only because of its history of addiction and abuse, but also because of its considerable central nervous system (CNS) and cardiovascular toxicity.4 The result of cocaine in conjunction with epinephrine in local injection can be catastrophic—leading to malignant hypertension and cardiovascular insufficiency if it prevents significant re-uptake of norepinephrine at nerve endings.
Many preparations for topical cutaneous applications are marketed for intact skin. Several nonprescription-strength formulations of lidocaine 4 to 5% are also available. EMLA (AstraZeneca Pharmaceuticals, LP, Wilmington, DE) is an oil-in-water emulsion of 2.5% prilocaine and 2.5% lidocaine that was approved by the Food and Drug Administration (FDA) in 1992.8 It works best when applied to the skin under an occlusive dressing for at least 45 to 60 minutes. LET (lidocaine 4%, epinephrine 0.1%, and tetracaine 0.5%), either as an aqueous solution or in a methylcellulose gel, is popular for laceration repairs. Standard dosage is 1 to 3 mL for ~ 20 to 30 minutes. The gel formulation may be applied directly onto the wound and surrounding skin without occlusion. Ultimately, we prefer to use our own topical preparation, which can be compounded as up to 30% lidocaine in Lipothene (LipoThene, Inc., Pacific Grove, CA). It provides quicker onset and is more effective than most other formulations.
Regional Blocks of the Face
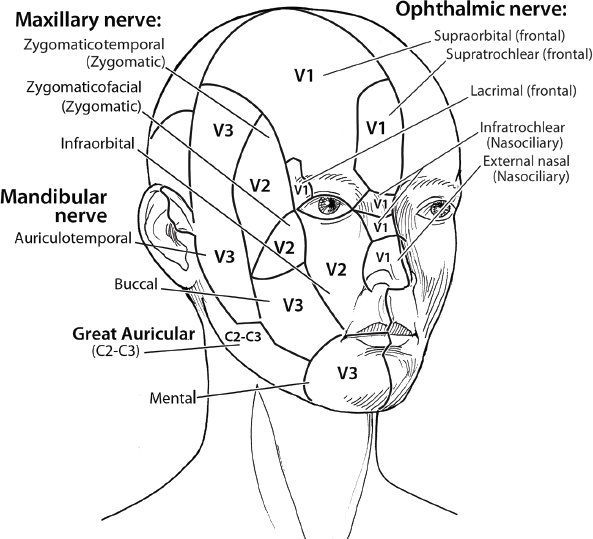
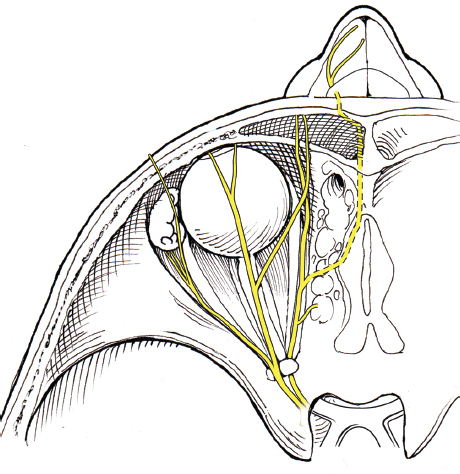
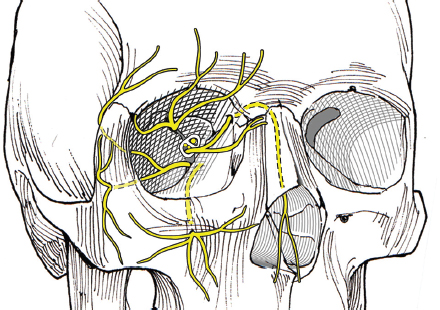
The trigeminal nerve (cranial nerve V) supplies sensory innervations to the face ( Fig. 4.1 ). Distributions of the trigeminal nerve can be further classified into three divisions: ophthalmic (V1), maxillary (V2), and mandibular (V3). The ophthalmic, maxillary, and mandibular branches exit the skull through three separate foramina: the superior orbital fissure ( Fig. 4.2 ), the foramen rotundum, and the foramen ovale, respectively. Within each division are several named nerves. Only the ones that are pertinent to regional blocks are addressed here ( Fig. 4.3 ).
Injection of local anesthetics does not have to be painful. There are several modifications that can be integrated to lessen the discomfort of injection. Cool solutions can be more painful than those at body temperature. Rapid infiltration also hurts more than slow injection. Addition of sodium bicarbonate will alter the pH of the anesthetic solution and help to attenuate the discomfort. Minimizing the number of injections by performing an effective regional block first will improve patient comfort. Addition of hyaluronidase will further help to accelerate the spread of the anesthetic and increase diffusion. Our standard technique utilizes 9 mL of 2% Xylocaine with 1:100,000 epinephrine mixed with 1 mL (150 units) of hyaluronidase.
Ophthalmic Division V1
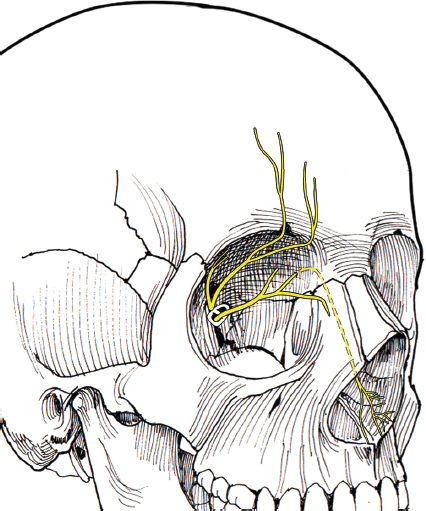
Supraorbital Nerve—Pertinent Anatomy
This nerve is located by the supraorbital notch, which is palpable in the supraorbital rim of the frontal bone ( Fig. 4.4 ). A vertical line can be drawn connecting this landmark with the infraorbital and mental foramen, which is a line drawn through the inner limbus of the eye. If measuring from the midline, this nerve reliably exits the skull between 2.5 and 2.7 cm. This measurement is important because the notch cannot always be palpated. In 60% of patients, the nerve is in the notch, whereas 32% of the time, it exits through a foramen. Supernumerary branches occur in 8% of all cases. After exiting, the nerve divides into two branches—a medial and a lateral. The medial branch runs on the surface of the frontalis; the lateral branch courses under the frontalis. There are instances where only the lateral branch exits from a separate foramen above the rim.9
Technical Aspects of Procedure
Inject 1 to 1.5 mL of local anesthetic under the edge of the superior orbital margin just lateral to the supraorbital notch Video 4.1.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


