4 Chest wall reconstruction with pectoralis major muscle flaps
INDICATIONS
Deep sternal wound infections
Mediastinitis following open heart surgery
Soft tissue coverage of large sternal defects following trauma or oncologic resection
Dehisced median sternotomy wounds
Intrathoracic dead space or bronchopleural fistula
Chest wall reconstruction
Head and neck reconstruction
INTRODUCTION
The pectoralis major flap was popularized in 1980 by Jurkiewicz for chest wall reconstruction; its most notable contributions have been in decreasing mortality and morbidity associated with sternal wound infections following open heart surgery. 1 The latissimus dorsi and rectus abdominus muscles are other local reconstruction options; however, the pectoralis muscle remains the workhorse flap for chest wall reconstruction due to its versatility. 2 The incidence of sternal wound infections or mediastinitis is approximately 1–5% following open heart surgery 3 and will typically increase length of hospitalization by 20 days and increase the cost by three times compared to an uncomplicated postoperative course. 4 , 5
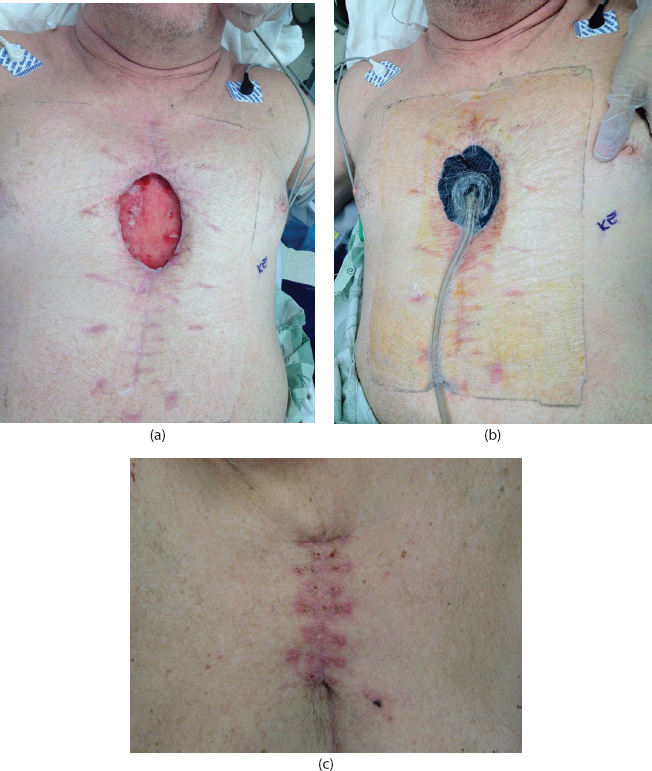
Keeping the reconstructive ladder in mind, local wound care does have its role in managing sternal wound infections. Patients with wound depth of less than 4 cm, negative blood cultures, and minimal sternal exposure or instability can be successfully managed with negative-pressure vacuum therapy (see Figure 4.1). The most important predictor of vacuum-assisted closure (VAC) success is wound depth less than 4 cm. 6
Numerous studies have shown that early coverage of sternal wounds with pectoralis flaps promotes wound closure and sternal stability. The most common indication for surgery is culture-positive median sternotomy wound dehiscence. 2 In a recent study reviewing 211 sternal wound infections, 95% of wounds were successfully closed with an overall mortality rate of 5.7%. Mortality rates for deep sternal wound infections prior to pectoralis coverage approached 50%. 7 , 8 Table 4.1 indicates the equipment necessary for this surgery.
PREOPERATIVE MARKINGS
Borders of the pectoralis (see Figure 4.2):
Superior: clavicle
Lateral: anterior axillary line
Medial: sternum
Inferior: sixth rib
The thoracoacromial artery arises from the midpoint of the clavicle and courses medially. The axis of the pedicle follows a line drawn from the acromion to the xiphoid. The thoracoacromial pedicle arises from the second portion of the axillary artery and travels underneath the pectoralis major in the subfascial plane.
INTRAOPERATIVE DETAILS
Introduction: There are several common variations of pectoral muscle flaps:
Advancement: The unipedicled pectoralis major advancement flap is based on the thoracoacromial artery. This will advance the overlying skin component along with the muscle (see Figure 4.3).
Turnover: The turnover pectoralis major muscle flap is based on the internal mammary artery (IMA) perforators penetrating rib spaces 2 through 5 (see Figure 4.4).
Combinations of all have been used for sternal reconstruction and closure with excellent results.
Due to the success of rotation/advancement flaps in this area, microvascular surgery is rarely necessary in sternal wound management.
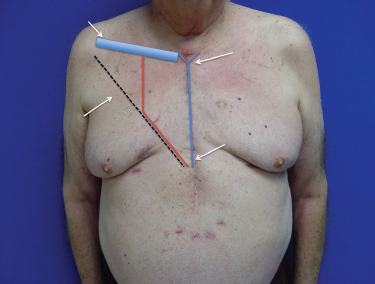
In planning a pectoralis flap, it is important to understand what vessels were used in cardiac surgery (see Figure 4.5).
The majority of bypass patients have at least the left and on occasion the right IMA harvested, limiting the use of the turnover pectoralis major muscle flap to one or neither side.
If the IMA is preserved, a turnover pectoralis flap is valuable as it fills the inferior defect of the chest wound.
For large sternal defects, one turnover flap is placed into the sternal defect, and the ipsilateral pectoralis is advanced for coverage.
This is also important for planning a rectus abdominus flap for sternal coverage.
Anesthetic requirements:
Appropriate resuscitation with blood or fluids.
Cardiac anesthesia if available is helpful.
Cardio-thoracic surgery as well as the pump team should be in the hospital if a cardiac emergency occurs during the procedure.
Maximal paralysis is helpful during the muscle harvest and closure.
Anatomy:
The pectoralis muscle is considered a Mathes and Nahai type V muscle flap with one dominant pedicle, the thoracoacromial artery, and several medial perforators originating from the IMA (Figure 4.6). The thoracoacromial artery provides the dominant axial supply to the pectoralis major and originates from the second part of the axillary artery, directly deep to the pectoralis minor, and courses laterally to reach the pectoralis major. This pedicle has little variability, and the whole muscle can be reliably raised without disrupting the underlying pectoralis minor.
The origin is the sternum, anterior surface of ribs 1 through 6, and the clavicle. The insertion is the bicipital groove of the proximal humerus.
Operative steps:
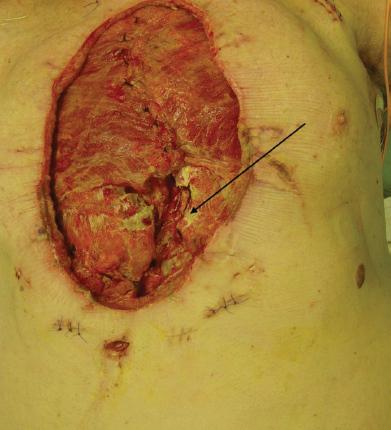
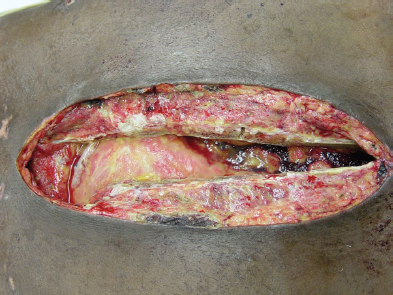
Debridement: The indication for pectoralis flaps often involves an infectious process; thus, thorough debridement of any infected or non-viable soft tissue, cartilage, or bone is the first step of the operation. Debridement of the wound is arguably the most important element to this operation as one of the most common postoperative complications is continued infection and dehiscence (Figure 4.7).
Removal of any skin, subcutaneous tissue, bone, or cartilage that is necrotic helps achieve sternal union and wound closure.
Irrigation with pulse lavage aids in decreasing the bacterial load of the wound (at least 3 L of saline with or without antibiotic or dilute iodine).
A rongeur and periosteal elevator allow for debridement of the affected sternum and cartilage.
Debridement and closure are usually done in stages, with initial deep intraoperative cultures to guide long-term antibiotics.
All foreign bodies, including sutures and sternal wires, must be removed to achieve a clean wound prior to closure.
Careful hemostasis must be obtained without the use of bone wax, which has been shown to increase the risk of persistent osteomyelitis.
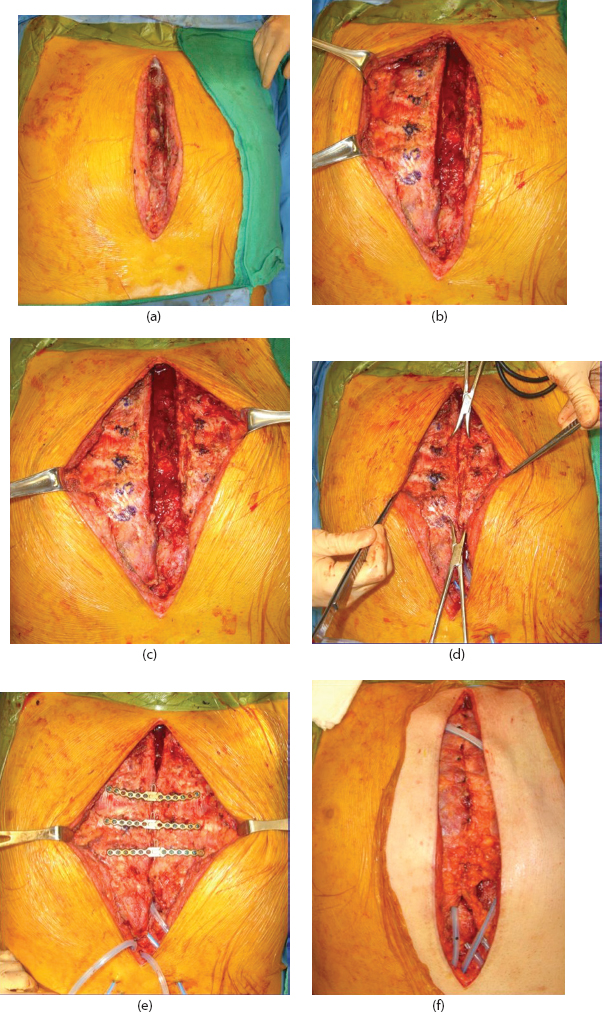
Considering sternal fixation (Figure 4.8): After debridement of the sternum and costal cartilage, there often remains a well-vascularized portion of bone that yields the opportunity for sternal fixation. 9 If viable bone and cartilage remain in the setting of paradoxical chest wall movement and sternal instability, rigid sternal fixation can be a part of chest wall reconstruction. 10 Rigid fixation offers the benefit of accelerated healing and sternal union while decreasing the incidence of mediastinal hernia. 11
Undermine the chest wall both superficial and deep to the pectoralis muscles. Preserve these muscles as they will be used as advancement flaps for sternal closure on top of the fixation system.
Identify at least three healthy ribs for the sternal fixation system.
Place bone fixation hooks on the edge of the sternum to allow for reduction.
Size the plates depending on rib size.
Place three or four plates on the ribs.
Use bicortical screws on the sternum and unicortical screws on the ribs. 12
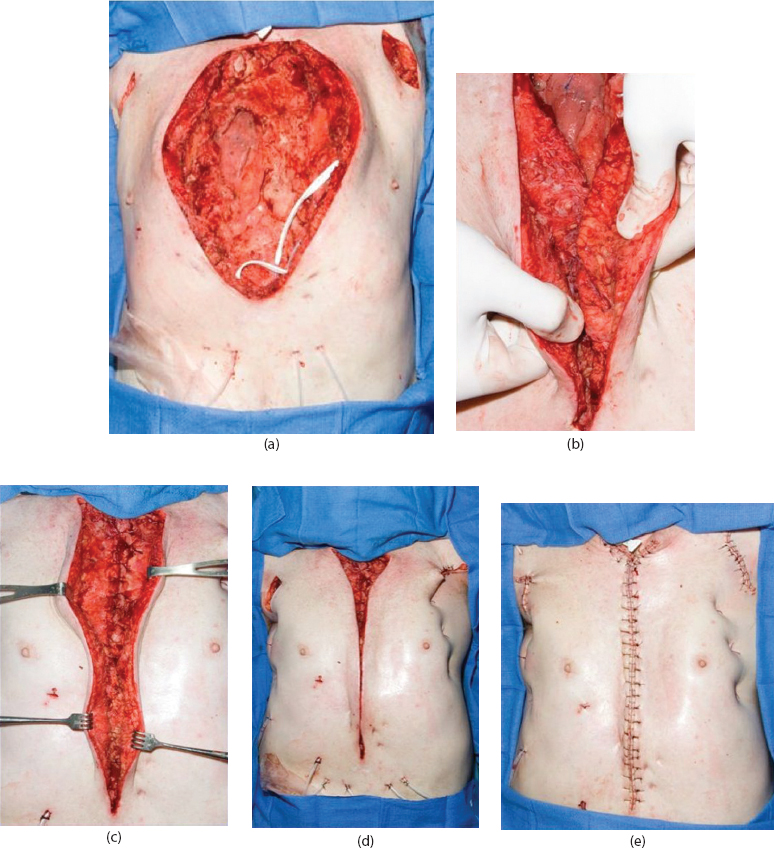
Myocutaneous advancement flaps (see Figure 4.3):
Minimal subcutaneous flaps are raised off the surface of the muscle from the midline sternal defect.
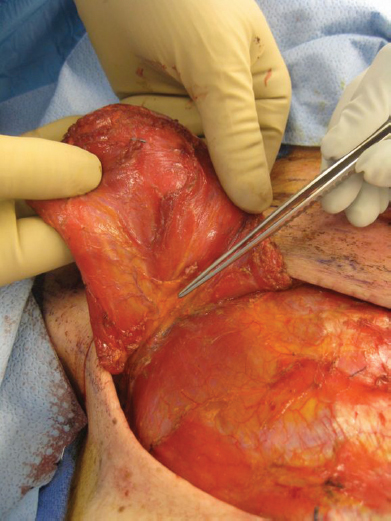
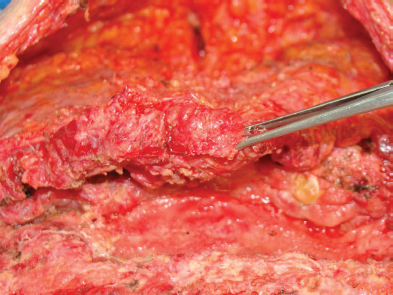
The muscle is elevated off the chest wall medial to lateral, taking care to ligate the intercostals and internal mammary perforators medially (Figure 4.9).
It is important to leave some perforators from the pectoralis muscle to the overlying skin to maximize healing potential and skin closure of the midline and to minimize the risk of seroma.
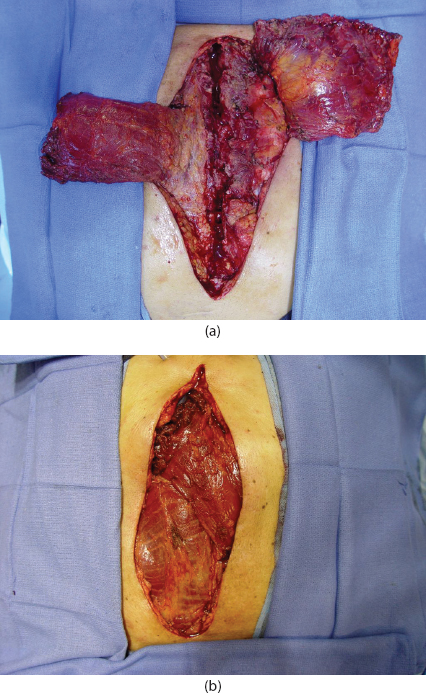
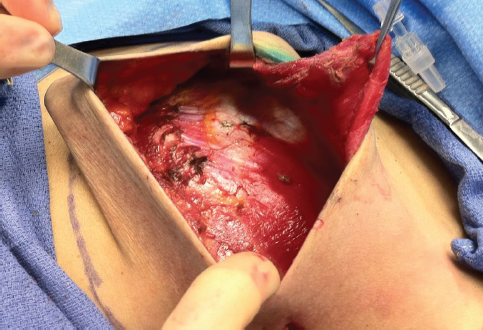
Care is also taken to avoid elevating the pectoralis minor with the flap (Figure 4.10).
There is a relatively avascular plane both superficial and deep to the pectoralis major muscles. By detaching the muscle from its sternal, rib, humeral, and medial clavicular attachments and separating it from the clavicular head of the deltoid, the pectoralis can usually be extended to the level of the xiphoid.
Lateral dissection at the insertion on the humerus may be done until the flaps reach midline without significant tension. This can be done through a separate incision near the humeral insertion.
If further advancement is needed caudally, back cutting the superior medial aspect of the pectoralis muscle up to 6 cm maintains its blood supply.
Another option for additional mobility involves detaching the sternocostal head from the clavicular head of the muscle.
When a significant amount of mediastinal dead space is a problem, bilateral flaps are usually necessary.
After the pectoral flaps have been raised, suture them in the midline with figure-of-eight sutures (strong monofilament such as 0-0 Prolene®; Ethicon, Somerville, NJ).
Place drains under flaps in the midline and under the bilateral subcutaneous undermined area.
Suture skin closed with horizontal mattress monofilament suture. Avoid buried sutures.
Use a light compression chest binder.
Turnover flaps (Figure 4.4):
The humeral insertion must first be divided. This can be done either by undermining the skin superficial to the muscle laterally over to the insertion or by a separate incision. A separate incision will commonly preserve chest skin viability.
Fold the lateral portion of the muscle into the mediastinum while maintaining its vascular supply by means of perforators from the IMA and anterior intercostal arteries. This maneuver may result in a contour deformity of the anterior chest wall, causing tension on the skin closure. However, it nicely fills dead space in the appropriately selected deep sternal wound.
One can also use a combination of the turnover pectoralis flap on the side in which the IMA has not been harvested and a unipedicled rotational advancement flap on the ipsilateral side.
The rotating end of the turnover flap may be sutured in place at the adjacent costal cartilage and intercostal fascia.
Close and place drains as described previously.
Use a light compression chest binder.
The disadvantage of the turnover flap is that the muscle is harvested on its non-dominant blood supply and if a midline sternotomy is needed again, the muscle may be damaged.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


