9 Breast reconstruction with abdominal flaps
INDICATIONS
Patients desiring autologous reconstruction
Patients with past history of radiation therapy
In patients following failed implant reconstruction
In patients who desire an “abdominoplasty” appearance
INTRODUCTION
Abdominal flap-based breast reconstruction remains a popular choice among patients seeking autologous breast reconstruction. This is primarily because the abdomen is often an excellent donor site, with a postoperative appearance resembling that of an abdominoplasty. Preservation of form and function is readily achieved using modern techniques of flap harvesting. The traditional transverse rectus abdominis myocutaneous (TRAM) flap requires the use of most, if not all, of the rectus abdominis muscle and has the potential disadvantage of abdominal weakness or abnormal contour abnormalities. With the advent of muscle preservation, donor site morbidities have been minimized using the muscle-sparing (MS) free TRAM, deep inferior epigastric perforator (DIEP), and superficial inferior epigastric artery (SIEA) flaps. These flaps, however, require expertise in microvascular techniques and thus are used occasionally based on national statistics. Table 9.1 indicates the equipment needed.
Handheld Doppler | Microvascular clamps |
Microscope and/or high-power loupes (>4×) | Sutures include: 3-0/4-0 Monocryl, 2-0 PDS, |
8-0 or 9-0 nylon suture | 0-Prolene® (Ethicon) |
Microsurgical instrument tray | 15-F drains |
Soft polypropylene mesh | Wide-mouth rongeur |
Vessel loupes | Thoracic set for internal mammary exposure |
Medium and small vascular clip appliers | Freer elevator |
Microclips | Heparinized saline |
Micro bipolar cautery | Electrocautery unit |
3000–5000 units of IV heparin prior to flap division | Short and long tenotomy scissors |
PREOPERATIVE MARKINGS
Breast markings
Superior extent of the breast is marked.
Inframammary fold is marked.
Midline is marked.
Lateral mammary fold is marked.
The mastectomy incisions are delineated (skin or NS pattern).
Abdominal markings
With the patient standing, the abdominal midline is delineated from the xiphoid process to the pubic bone. The anterior superior iliac spine (ASIS) is palpated and delineated bilaterally. The proposed upper border of the flap is delineated. This definitive line is marked at the level just above the umbilicus. The inferior extent of the flap is marked via a curvilinear line extending from the ASIS toward the pubic symphysis. This line is tentative and is not definitively decided on until the patient is in the operating room (Figure 9.1).
Observation for an abdominal hernia or diastasis is important, as the recti muscles will be slightly laterally displaced.
Handheld Doppler verification in the peri-umbilical area is sometimes useful and can isolate the location of potential perforators.

INTRAOPERATIVE DETAILS
Free MS-TRAM/DIEP/SIEA flaps: Common pathway
The approach to the patient desiring free-tissue transfer is considerably different from that for a pedicled transfer. Therefore, a pedicled abdominal flap is discussed in a different section.
The superior incision is initially made down to the level of the anterior rectus sheath. This plane is dissected superiorly using electrocautery to the level of the xiphoid process and costal margin.
The patient is flexed approximately 30°, and the undermined upper abdominal flap is transposed over the lower abdominal pannus to confirm the position of the inferior incision. This maneuver will ensure that the abdomen will be able to be closed.
Once confirmed, the entire ellipse is incised using electrocautery to the level of the anterior rectus sheath.
If the SIEA and vein are visualized and of appropriate caliber, an SIEA flap can be considered. These vessels are usually located in the paramedian region of the inferior incision.
SIEA pathway
Dissection of the vessels in the SIEA pathway is performed using a combination of sharp and blunt instruments. Once sufficient length is achieved, the flap is ready for harvest.
MS free TRAM or DIEP pathway
If the SIEA flap is not possible because the vessels are absent or inadequate, the MS free TRAM or DIEP flap algorithm is followed.
A circumferential incision around the umbilicus is made, and the umbilicus is preserved on its stalk.
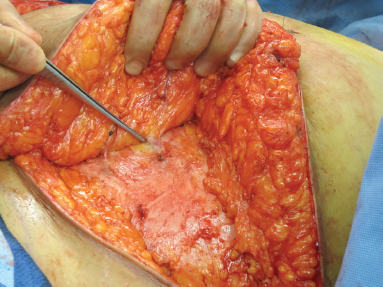
The initial dissection proceeds lateral to medial, extending to the linea semilunaris. Medial to the linea semilunaris requires careful dissection using either low-energy monopolar cautery or bipolar cautery to look for the perforating vessels from the deep inferior epigastric system.
At this point, a critical decision is made regarding the MS free TRAM or the DIEP flap. If the patient’s body habitus permits and the presence of a dominant perforator with a palpable pulse is verified, a DIEP flap dissection is performed (Figure 9.2).
Related posts:
 7 Implant-based breast reconstruction: Tissue expander placement after mastectomy
7 Implant-based breast reconstruction: Tissue expander placement after mastectomy
 5 Breast reduction: Inferior pedicle, wise pattern
5 Breast reduction: Inferior pedicle, wise pattern
 8 Implant-based breast reconstruction: Exchange of tissue expander for permanent implant
8 Implant-based breast reconstruction: Exchange of tissue expander for permanent implant
 10 Nipple reconstruction
10 Nipple reconstruction
 6 Gynecomastia
6 Gynecomastia
 1 Skin grafting and dermal substitute placement
1 Skin grafting and dermal substitute placement
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


