10 Nipple reconstruction
INDICATIONS
Nipple reconstruction is indicated for reconstruction after partial or complete nipple loss due to the following:
Mastectomy
Necrosis due to complications of breast surgery
Techniques:
Modified skate flap with a full-thickness skin graft: Indicated for reconstruction of the nipple on mastectomy skin flaps
Purse-string modified skate flap: Indicated for reconstruction of nipple on a thicker native breast mound or tissue flap skin paddle
Contralateral nipple sharing: Indicated for single-nipple reconstruction with a large native contralateral nipple
Skate flap with primary closure: Indicated for nipple reconstruction with modest projection and no additional donor site
INTRODUCTION
There are several successful techniques for nipple reconstruction that produce acceptable results. It is the senior author’s experience that techniques that use local flaps and primary closure result in significant loss of projection over time for several reasons: First, the size of the flaps is often compromised to allow for closure. Second, the force of the scar contracture over time pulls on the reconstructed nipple, limiting the projection. In contrast, use of a full-thickness graft or purse-string modification allows for generous flaps to be created that can effectively take into account the inevitable loss of size over time. Although the purse-string modification can provide generous amounts of flap tissue, it requires fairly thick flaps (either a flap skin paddle or thick mastectomy flaps) to ensure adequate vascular supply to the fully released areolar and skate flaps. For these reasons, the modified skate flap with a full-thickness skin graft is our primary reconstructive technique in the setting of implant-based reconstruction. The purse-string modification of the skate flap is our primary reconstructive technique when a skin paddle is present. Equipment is listed in Table 10.1.
1% lidocaine with epinephrine 1:100,000 Curved tenotomy or face-lift scissors #11 blade scalpel Smooth needle drivers (3) 5-0 nylon 5-0 chromic Vaseline gauze, 5 × 9 Sterile cotton balls Sterile 4 × 4 gauze |
MODIFIED SKATE FLAP WITH FULL-THICKNESS SKIN GRAFT
Preoperative markings
The patient is always marked in the upright position.
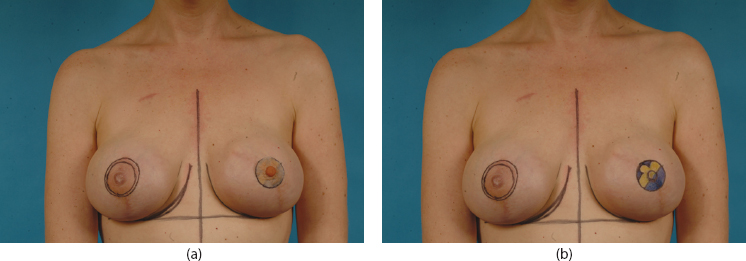
The position of the reconstructed nipple-areolar complex (NAC) must be determined first. In the case of unilateral reconstruction, symmetry with the contralateral NAC will determine the location. In bilateral reconstruction, the new NAC positions will be placed symmetrically at the point of maximal projection of the breast. We utilize prosthetic nipples or electrocardiograph (ECG) patches to guide positioning of the new NAC(s) (Figure 10.1a).
A 40- to 44-mm areolar diameter is traced at the identified NAC site. The center of the areola is marked with a 5- to 10-mm diameter circle, which represents the position of the nipple.
A modified skate flap is diagramed, creating wings approximately 1 cm wide on both sides and a mosque-shaped cap. The base, which is the vascular pedicle, should remain approximately 1 cm wide and be oriented to maximize vascular supply. In other words, the pattern may be rotated to position the base toward a scarless area of the mastectomy skin, which optimizes the blood flow. The pattern should be slightly off center, skewing the entire design toward the cap, as it will be pulled toward the base of the flap when elevated (Figure 10.1b).
The 40- to 44-mm areolar pattern is traced into a groin crease for harvest of a full-thickness skin graft. To allow for removal of the dog-ear, an elliptical pattern is drawn around the identified graft, following the relaxed skin tension lines. Alternatively, any pre-existing scar line on the abdomen or back may be used as the donor site.
Intraoperative details
The breast and groin patterns are infiltrated with 1% lidocaine with epinephrine 1:100,000.
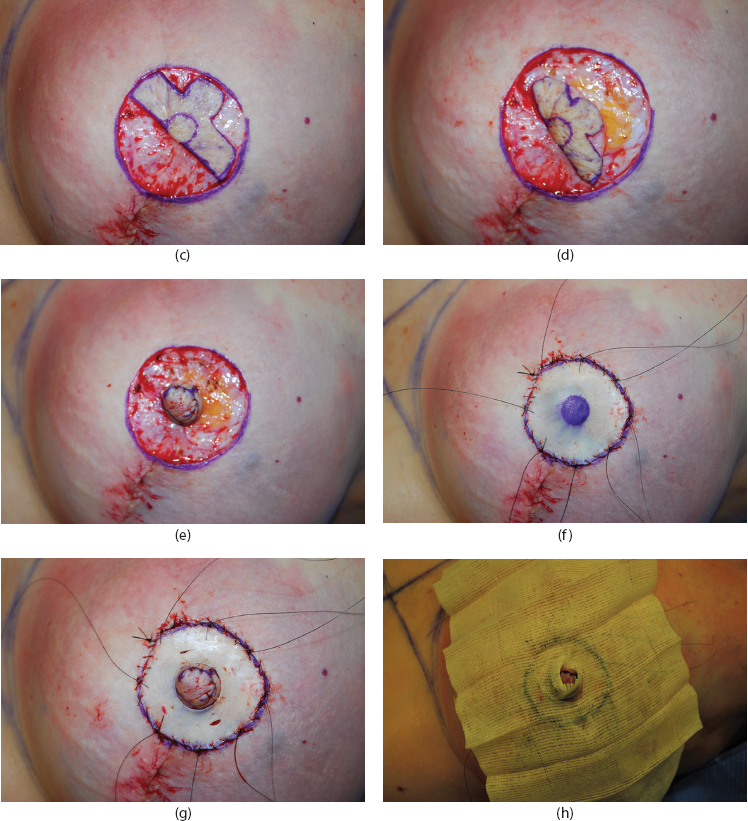
The entire NAC pattern is incised through epidermis only. The portion of the areola surrounding the skate flap is de-epithelialized superficially (Figure 10.1c). The skate flap is raised, retaining a thin, even layer of fat on the undersurface of the flap (Figure 10.1d). Care is taken to leave the base and the associated vascular supply intact. The pattern is elevated until the wings easily wrap around the pattern without tethering.
The skate-flap wings are approximated end to end, and the cap is draped onto the approximated wings. This is sutured with interrupted 5-0 chromic sutures (Figure 10.1e).
The full-thickness skin graft is harvested from the groin, taking the circular areolar pattern first and then removing the surrounding ellipse.
The graft is thinned meticulously with curved scissors until it is a thin full-thickness graft that is nearly transparent.
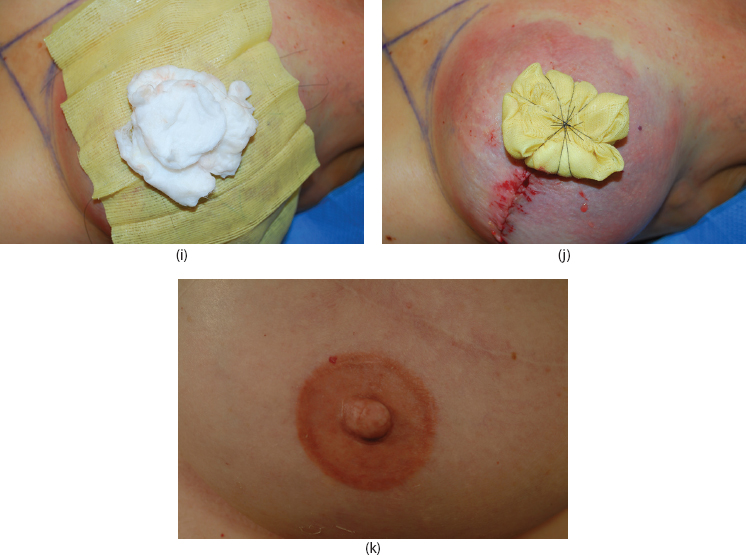
The graft is sutured over the nipple reconstruction with interrupted 5-0 nylon sutures equally divided at eight cardinal points, and the tails are left long to function as a bolster tie-over. A running 5-0 nylon suture is used to secure the entire diameter of the graft.
A circle of the same size as the reconstructed nipple is marked on the center of the graft and excised with curved scissors (Figure 10.1f). The reconstructed nipple is exposed through this perforation in the graft. The base of the nipple is sutured to the graft with interrupted 5-0 chromic sutures. An 11 blade is used to piecrust the graft and allow for serous drainage, which can impede graft take (Figure 10.1g).
Related posts:
 7 Implant-based breast reconstruction: Tissue expander placement after mastectomy
7 Implant-based breast reconstruction: Tissue expander placement after mastectomy
 5 Breast reduction: Inferior pedicle, wise pattern
5 Breast reduction: Inferior pedicle, wise pattern
 8 Implant-based breast reconstruction: Exchange of tissue expander for permanent implant
8 Implant-based breast reconstruction: Exchange of tissue expander for permanent implant
 9 Breast reconstruction with abdominal flaps
9 Breast reconstruction with abdominal flaps
 6 Gynecomastia
6 Gynecomastia
 1 Skin grafting and dermal substitute placement
1 Skin grafting and dermal substitute placement
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


