2 Component separation
INDICATIONS
Large ventral hernias that cannot be closed primarily by apposition of the anterior rectus sheath
Large abdominal wall defects after extirpative surgery or flap harvest that cannot be closed primarily by apposition of the anterior rectus sheath
INTRODUCTION
Large abdominal hernias pose a reconstructive challenge. Component separation provides a means of recruiting innervated, vascularized autologous tissue for closure of ventral hernias or for immediate closure of large abdominal wall defects resulting from resection of the midline rectus abdominis complex or harvest of a vertical rectus abdominis myocutaneous (VRAM) flap. Key to successful surgery is thorough understanding of the anatomy of the anterior abdominal wall. Release of the external oblique muscles and the posterior rectus sheath allows the paired rectus abdominis muscles to come together in the midline to form a dynamic muscular sling (Figure 2.1). Special equipment for the procedure is shown in Table 2.1.
Warm saline bath not to exceed 37°C Cefoxitin 2 g IV given prior to incision Jackson-Pratt #10 flat drains, 2 per side Sterile antiseptic skin preparation Choice of synthetic versus biologic mesh |
PREOPERATIVE MARKINGS
Lateral border of rectus abdominis muscle (semilunaris line)
Anterior superior iliac spine
Inguinal ligament
Inferior margin of the ribs
External oblique muscles
INTRAOPERATIVE DETAILS
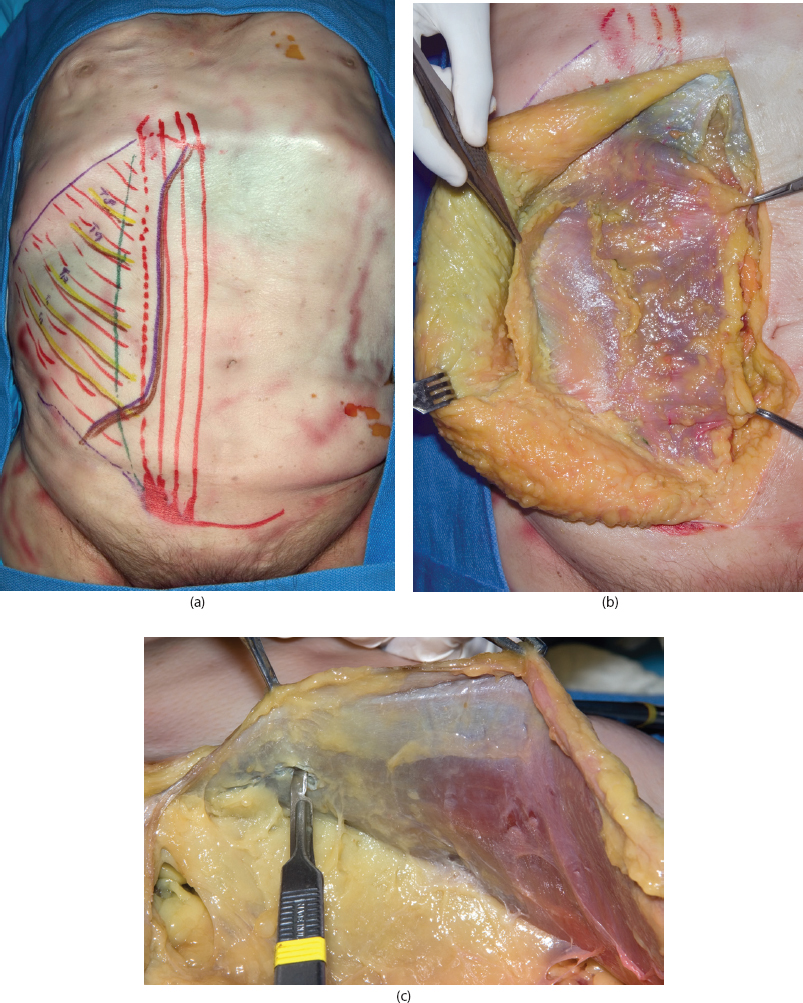
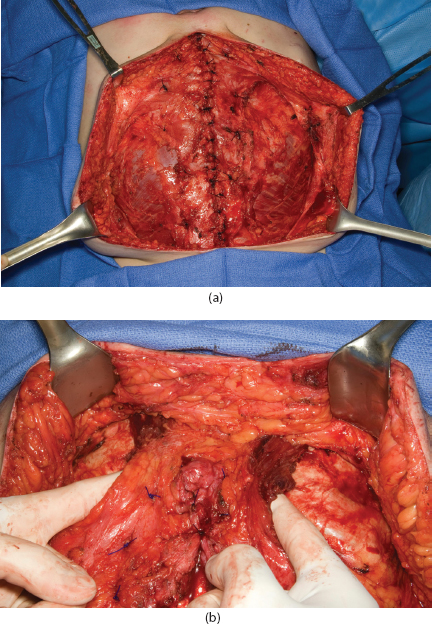
Incision is made on the margin of the skin graft or scar tissue overlying the ventral hernia (Figure 2.1a and b).
Sharp dissection laterally is used to undermine the skin and subcutaneous tissue over the abdominal wall (anterior rectus sheath medially, then external oblique laterally). Care is taken to prevent inadvertent enterotomies.
If a skin graft overlies the hernia, it is removed with a #10 blade. If the surgeon is not confident that closure of the hernia is possible, the skin graft is left in place until it is clear that closure is possible. Care is taken not to injure the underlying intestine. If an enterotomy is made, it must be recognized and closed. Copious irrigation is performed. In the case of an enterotomy, we avoid use of prosthetic mesh; biologic mesh can be used.
The dissection is carried laterally up to 6 to 10 cm lateral to the semilunar line.
The semilunar line is identified and marked. A longitudinal line is marked 2 cm lateral to the semilunar line running 5 to 10 cm above and 5 to 10 cm below the level of the hernia. An incision is made through the external oblique fascia. The external oblique is separated from the internal oblique muscle and fascia medially to laterally to the midaxillary line.
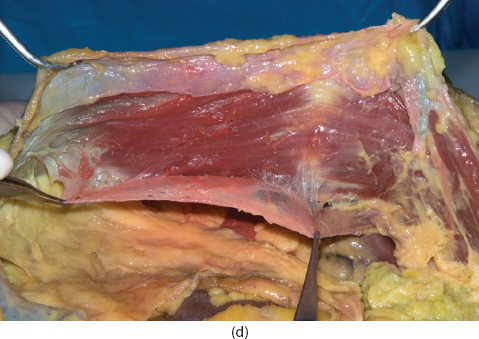
For hernias that extend close to the xiphoid, advancement of the rectus muscles medially can be a challenge. In these cases, the incision through the external oblique is extended above the ribs and then goes in an oblique fashion across the anterior rectus sheath. The rectus muscle is undermined over the ribs and advanced medially (see Figure 2.2a and b). Care is taken to identify the deep superior epigastric vessels so they are not injured during dissection.
Release of the external obliques bilaterally allows advancement of approximately 3 to 5 cm in the upper third of the abdominal wall, 7 to 10 cm in the middle third, and 3 cm in the lower third.
Adequacy of release and residual tension are assessed by pulling the paired rectus abdominis muscles to the midline.
Excess skin and scar overlying the ventral hernia are excised.
Another component of the release involves a longitudinal cut in the posterior rectus sheath (Figure 2.1c and d). Intestinal tissue and adhesions are released from the posterior rectus sheath all the way lateral to the lateral margin of the rectus muscles. Going further laterally is beneficial in most circumstances to be able to secure a piece of mesh if that is to be used. A line is marked on the posterior rectus sheath 2 cm lateral to the medial margin of the rectus muscle. An incision is made in the posterior rectus sheath. The posterior rectus sheath is then separated from the rectus muscles medially to laterally to the lateral margin of the rectus muscle. This allows further advancement of approximately 2 cm in the upper third of the abdominal wall, 2 to 4 cm in the middle third, and 2 cm in the lower third.
The intraperitoneal cavity is irrigated with warm saline prior to closure.
The midline structures (medial edge of the rectus fascia) are brought together using running #1 PDS® sutures (polydioxanone, Ethicon, Norderstedt, Germany).
If the posterior rectus sheath can be approximated, then a prosthetic or biologic mesh is placed in the retrorectus space followed by approximation of the rectus muscles.
If the posterior rectus sheath cannot be approximated, a large piece of prosthetic or biologic mesh is placed in the abdominal cavity as an underlay spanning the abdominal wall from the anterior axillary line on one side to the anterior axillary line on the other side and from the inferior rib margin cephalad to the iliac spine caudad.
If the anterior rectus sheath and rectus muscles will not come together in the midline, a biologic or prosthetic mesh is placed as an underlay to the abdominal wall. Another piece of mesh can be used as an inlay or overlay as well to support the repair. This is anchored to the anterior rectus fascia with multiple horizontal mattress sutures using #1 PDS suture. If biologic mesh is used, Strattice™ (LifeCell™, Branchburg, NJ) is preferred to AlloDerm® (LifeCell) as it has a decreased capacity to stretch. Synthetic mesh should be avoided if the surgical site is contaminated and in patients with comorbidities that cause an unacceptably high risk for developing surgical site infection. Often, following anchoring of the underlay, the anterior rectus sheath can be closed in the midline due to redistribution of tension.
The anterior rectus sheath is then apposed using multiple #1 or 0 PDS sutures placed in a vertical or figure-of-eight mattress fashion.
Two #10 flat Jackson-Pratt (JP) drains are placed on each side to drain the subcutaneous pocket.
The skin is closed in layers.
A petroleum-based ointment is placed over the incisions, followed by a dressing. An abdominal binder is applied for support, particularly when the patient is ambulating or coughing. In patients with a large pannus, we will use a Steri-Drape™ (3M™, St. Paul, MN) placed from one side of the abdominal wall to the other while taking tension off the midline incision. One person will come from the lower end and use both hands to bring the pannus together from one side of the patient to the other. The Steri-Drape is placed on the abdominal wall while the pannus is squeezed in the midline. This allows for the tension to be on the Steri-Drape instead of the midline incision. Multiple layers of Steri-Drape can be placed. This is removed in 2 to 3 days. Maceration of the skin does occur with this type of dressing.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


