36 Management of the Middle Vault
Introduction
Management of the middle vault in rhinoplasty was for many years considered little more than removal of a hump deformity. The traditional reduction rhinoplasty often included sharp resection of the middle vault apex (cartilage and mucosa) with little regard to nasal function or longterm sequelae. In the 1980s, surgeons began to recognize longterm complications of this approach, including functional nasal obstruction and aesthetic deformity. 1 Increasing importance is now placed on preventive measures in primary rhinoplasty to avoid these problems and reconstructive techniques to repair damaged middle vaults. 2 In this chapter we describe these techniques and identify patients who are at risk for middle vault pathology during rhinoplasty.
Middle Vault Anatomy
Beneath the nasal skin and soft tissue, the middle vault is composed of the paired upper lateral cartilages and the dorsal nasal septum. Superiorly, the upper lateral cartilages are fused with the nasal bones, inserting approximately 2–3 mm cephalic to the caudal margin of the bones. Medially, the upper lateral cartilages fuse with the cartilaginous septum; caudally, the cartilages separate from the septum and are relatively mobile. The caudal ends of the upper lateral cartilages have recurvature or scroll regions with attachments to the lower lateral cartilages. Laterally, the upper lateral cartilages approach the rim of the pyriform aperture, fusing with dense fibrous tissue. The mucosa is tightly attached to the internal surface of the upper lateral cartilages and is continuous with the lining of the septum and lateral nasal wall ( Fig. 36.1 ). When exposing the nasal structures during rhinoplastic surgery, dissection and undermining of the nasal soft tissues should be performed deep to the superficial musculoaponeurotic system to prevent devascularization and thinning of the overlying skin–soft tissue envelope. To preserve the structural support of the keystone region, care should be taken to ensure the upper lateral cartilages are not disarticulated from caudal nasal bones.
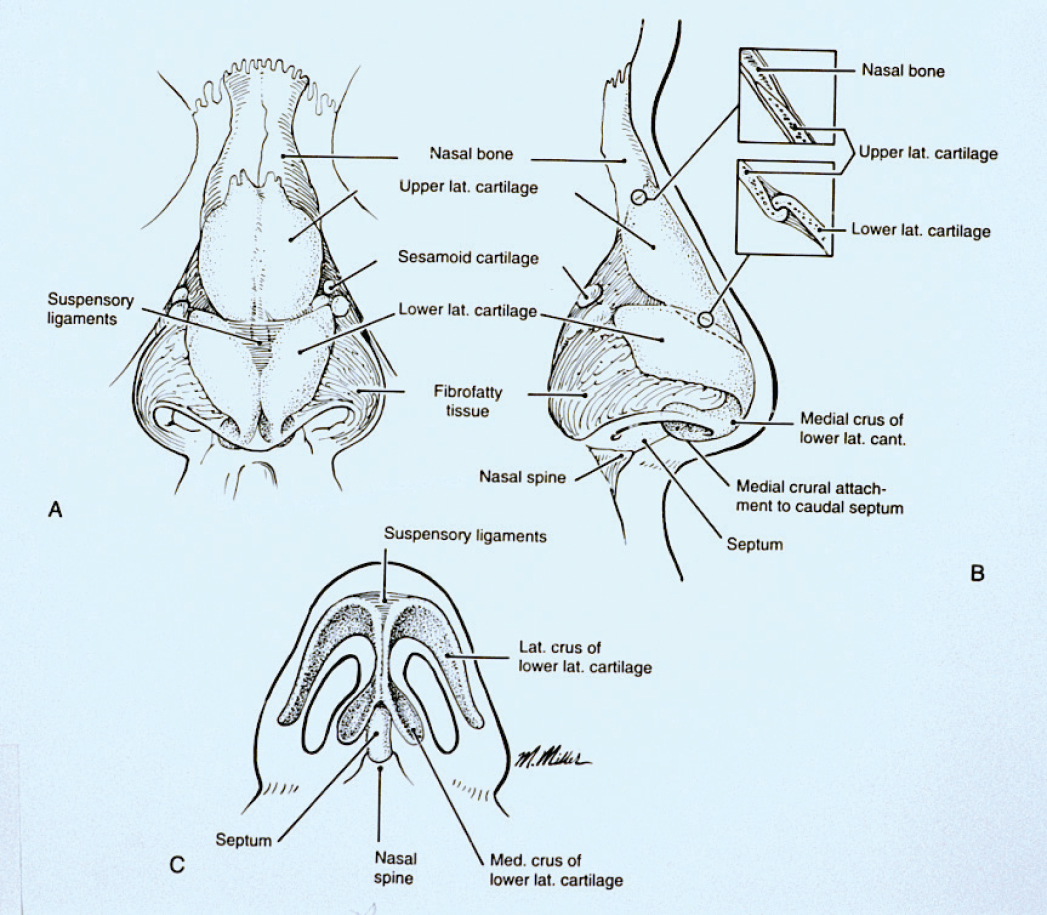
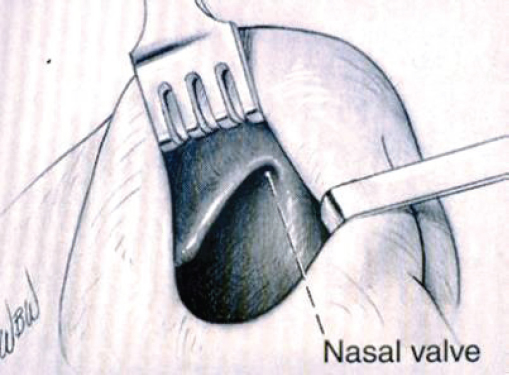
The internal nasal valve is defined by the caudal margin of the upper lateral cartilage superolaterally, the bony pyriform aperture laterally, the septum medially, the floor of the nose inferiorly, and the anterior head of the inferior turbinate posteriorly. This region is the narrowest part of the nasal passage with a crosssectional area of 55 to 83 mm2, and is thus the site of highest airflow resistance. 3 The angle between the septum and the upper lateral cartilage has a normal range of 10 to 20 degrees, and narrowing of this angle due to trauma, surgery, or disease can cause significant nasal obstructive symptoms ( Fig. 36.2 ).
Significance of Middle Vault Anatomy in Rhinoplasty
Middle vault complications are among the most significant concerns that trouble patients after rhinoplasty. Five to 15% of rhinoplasty patients ultimately undergo revision surgery, 4 , 5 and middle vault issues are two of the three most common reasons leading to the need for revision surgery. 6 Historically, reduction rhinoplasty has been found to decrease the crosssectional area of the internal nasal valve by 25%. 7 , 8 Recently, there has been an increased emphasis on anticipating middle vault anatomy and factors that lead to nasal valve complications. This improves patient outcomes and satisfaction after rhinoplasty. 2 , 9
Many reduction rhinoplasty techniques can disrupt the structural integrity and support of the middle vault. Dorsal hump reduction is one of the most common maneuvers that result in destabilization of the middle vault. Traditionally, the cartilaginous hump was excised en bloc with the underlying mucosa. This technique causes separation of the upper lateral cartilages from the septum and disruption of the underlying mucoperichondrium. This, in turn, leads to inferomedial collapse of the upper lateral cartilages, which is worsened if the mucosa is also incised. 10 Consequently, the middle vault is destabilized, which can result in the inability to withstand contractile healing forces or the inward pressure of inspiration. During a dorsal hump reduction, if dorsal and caudal septal struts of 10 mm in width are not preserved, the risk of middle vault collapse and saddle deformity is greatly increased. When performing a septoplasty, if a strut of at least 10 mm is not initially preserved, subsequent hump reduction can result in an insufficient dorsum and a weakened middle vault. Future scar contraction will cause loss of support leading to middle vault changes.
Telltale cosmetic deformities of middle vault instability (inverted-V, crooked middle vault, overly narrowed middle vault) and symptomatic internal nasal valve obstruction can become apparent immediately or gradually over a period of years. Changes can occur several years into the postoperative period as a result of continued contraction of the soft tissue envelope against a weakened cartilage skeleton. The classic inverted-V deformity is a result of destabilized upper lateral cartilages migrating posterior and inferior, allowing the caudal edges of the nasal bones to become visible externally. Identifying risk factors prior to rhinoplasty and utilizing surgical techniques to stabilize the middle vault during the procedure may prevent these troublesome postoperative issues.
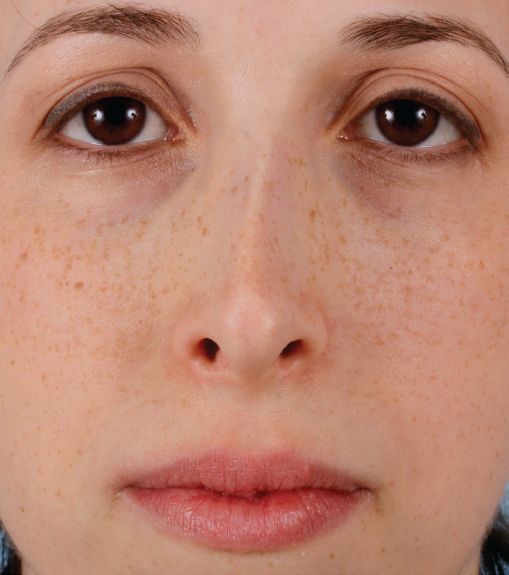
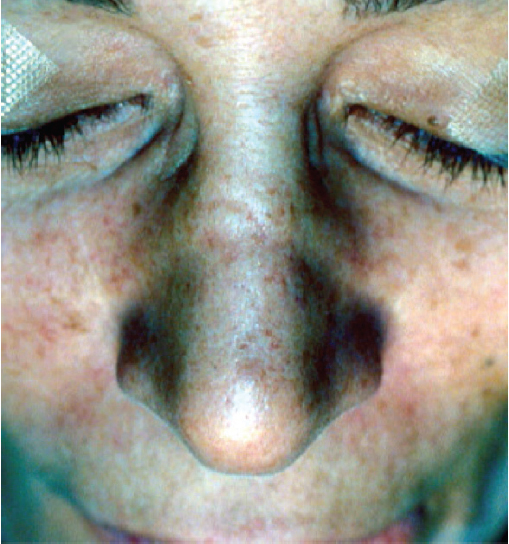
In addition to surgical etiologies of middle vault problems, there are several other conditions that may precipitate internal nasal valve obstruction. Through loss of nasalis muscle function, facial paralysis can lead to ptosis of the lateral nasal soft tissues and narrowing of the valve, causing symptomatic obstruction. Cancer resection of the lower twothirds of the nose may lead to scar contraction and distortion of the valve. In addition to nasal surgery, autoimmune diseases and intranasal drug use are other causes of severe middle vault collapse and saddle nose deformity. Senile tip ptosis can also cause significant narrowing and nasal obstruction. In these cases specialized surgical treatment can lead to improved quality of life ( Fig. 36.3 ).
Recognizing Risk Factors and Preventing Middle Vault Problems in Rhinoplasty
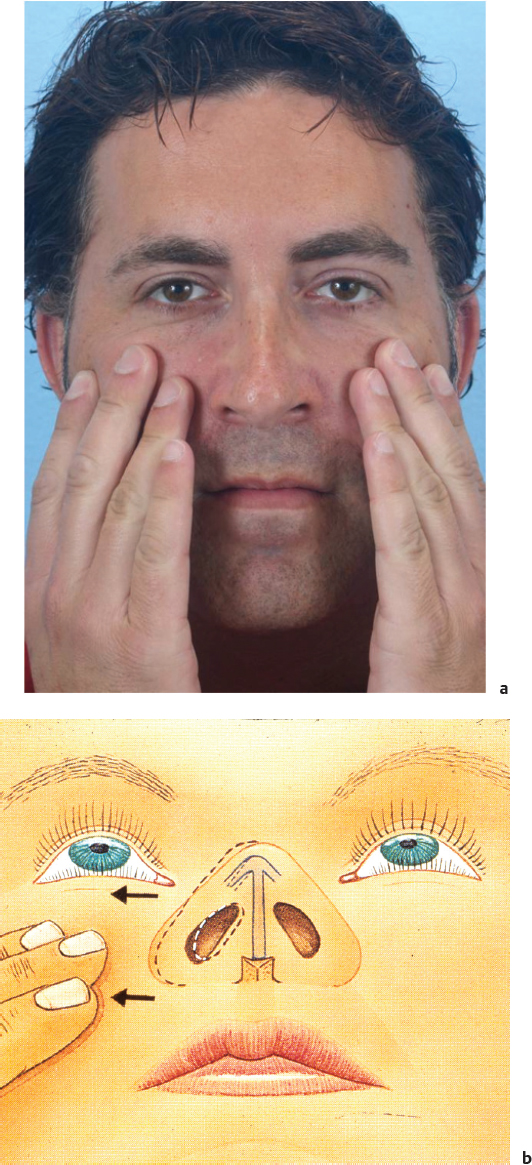
The most common problems of the middle vault include internal nasal valve collapse or stenosis, inverted-V deformity, middle vault dorsal asymmetry, and overnarrowing of the dorsum. Rhinoplasty surgeons must be able to evaluate the middle vault of each patient individually to determine the risk of postoperative issues. Not every patient is at risk for iatrogenic middle vault pathology. Patients with wide middle vaults can often undergo dorsal hump reduction and narrowing of the internal nasal valve without the need for middle vault reconstruction; this is particularly true in the African American population. However, the surgeon must be able to identify patients with risk factors in whom further narrowing without careful consideration is ill advised. Proper preoperative evaluation and planning prevent most middle vault complications. Highquality photographs provide invaluable information and should be studied prior to surgery. Specific risk factors have been identified as predisposing to middle vault problems in rhinoplasty including short nasal bones, long and weak upper lateral cartilages, thin skin, tall and narrow noses, previous trauma or surgery, preoperative positive Cottle test, tension nose deformity, and anteriorly positioned inferior turbinates ( Fig. 36.4 ). 11 , 12
In patients with the above risk factors for postoperative middle vault issues, preventive adjunctive techniques should always be considered. These include preservation of middle vault support structures, judicious resection in dorsal hump reduction, use of conservative osteotomies, and reconstruction of the cartilaginous middle vault structural support with cartilage grafting. Rhinoplastic surgeons should employ as many of these techniques as are required to ensure a stable middle vault that will withstand the inevitable forces of scarring and wound contraction over time.
Whenever possible, middle vault support structures should be preserved. Aggressive rasping of the bony dorsum should be avoided to prevent inadvertent disarticulation of the upper lateral cartilages from the nasal bones and destabilization of the middle vault. Interruption of the scroll region or resection of the upper lateral cartilages should be performed with caution. Toriumi and Johnson 11 have demonstrated that preservation of the middle vault mucosa helps to minimize posterior displacement of the upper lateral cartilages during hump removal. This mucosal bridge between the septum and upper lateral cartilages is preserved by the creation of junction tunnels under the attachment area of the septum and upper lateral cartilage. Preservation of this mucosa also helps to maintain a bloodless surgical field.
When performing dorsal hump reduction, resection should be conservative. Maintenance of a strong dorsal line is usually desirable for both aesthetic and functional reasons. In a patient with dorsal convexity and a narrow vault, it may be necessary to reduce the dorsum minimally, widen the middle vault with spreader grafts, and increase tip projection to achieve nasal harmony.
Overnarrowing of the nose due to medial displacement of the nasal bones after aggressive osteotomies is a common postoperative problem that should be avoided. Although many rhinoplasty patients desire a narrower nose, overly aggressive narrowing may decrease the distance between the lateral nasal wall and the septum, medializing the upper lateral cartilages and narrowing the internal nasal valve.
Grymer’s cadaveric study showed that lateral osteotomies resulted in a 12% reduction in the total minimum crosssectional area and a 15% reduction in the crosssectional area at the pyriform aperture. 13 Guyuron similarly found that osteotomies constricted the nasal airway in the majority of cases, with the most significant airway narrowing found in patients with anteriorly positioned inferior turbinates and significantly medializing osteotomies. 14 To reduce the risk of airway narrowing, osteotomies should be relatively conservative, and the soft tissue attachments of the nasal bones and upper lateral cartilages should be preserved ( Fig. 36.5).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


