34 Outcomes and Tumor Recurrence After Oncoplastic Surgery of the Breast: Eighteen-Year Follow-up
Oncoplastic surgery may allow more-extensive resections and good aesthetic outcomes in some patients, minimizing the deformity and expanding the indications for breast-conserving therapy (BCT). 1 Although numerous series have documented acceptable cosmetic outcomes using these techniques, the available data on local recurrence and distant metastasis following oncoplastic surgery are limited. Most series are small, with a relatively short follow-up.
In this chapter we first review our experience with 148 consecutive patients who underwent oncoplastic surgery consisting of BCT and concomitant bilateral plastic remodeling. We also present an updated follow-up of our cohort, 18 years after the original procedure. Local recurrence, metastases, and death rates are reported. Related complications and cosmetic outcomes are also discussed. All patients are reclassified according to the Revision of the American Joint Committee on Cancer staging system for breast cancer. 2
Surgical Approach
The oncoplastic procedures were performed with the patients under general anesthesia. Using a two-team approach, oncologic and plastic surgeons worked on both breasts simultaneously.
The tumor resection included at least 1 cm of macroscopically safe margin.
If the lesion was close to the resection margins, further resection was performed. The deep and superficial surfaces of the remaining breast tissue were evaluated bimanually for occult lesions. 3 , 4 The mammaplasty techniques used to reconstruct the involved breast were superior pedicle (Lejour or Pitanguy techniques), inferior pedicle, round block, latissimus dorsi, or definitive silicone implants. 5 – 7 The contralateral mammaplasty was performed concomitantly in all cases of this series, with a technique similar to that used in the breast with the tumor to achieve the best symmetry. A complete axillary dissection or sentinel node biopsy was performed in all clinically indicated cases, independent of the oncoplastic technique. When the sentinel node was positive after an extensive frozen section analysis, a complete axillary dissection was performed according to our previously described protocol. 8
Histopathologic Examination
Specimens were weighed and well oriented in the operating room to allow the pathologist to evaluate the margins grossly or microscopically to determine the need for further treatment and eventual reexcision. The volume of each specimen was calculated by multiplying the length, width, and height. 9 They were inked and formalin fixed, and paraffin-embedded sections were stained with hematoxylin and eosin for routine examination.
For consistency with the literature, we used a 2 mm surgical margin as the cutoff point for negative margins.
Positive margins were defined as those with tumor cells at the cut edge of the specimen. Close margins were defined as those with tumor cells between the cut edge of the specimen and the boundary defined as negative (less than or equal to 2 mm).
A complete axillary dissection or sentinel node biopsy was performed in all clinically indicated cases, independent of the oncoplastic technique. When the sentinel node was positive after an extensive frozen section analysis, a complete axillary dissection was performed according to our previously described protocol. 8
Adjuvant Treatment
The decision-making process to use adjuvant systemic therapy (hormone therapy or chemotherapy) was based on the clinical and pathologic statuses, and the therapy followed our standard protocols, without modification. All chemotherapy regimens began 15 to 45 days after surgery. We followed four chemotherapy schedules in this series of patients:
Cyclophosphamide, methotrexate, and fluorouracil (CMF)
Anthracycline plus cyclophosphamide (AC)
Four cycles of AC and three cycles of CMF (AC and CMF)
High-dose chemotherapy with autologous stem cell transplantation rescue.
Anthracycline regimens or high-dose chemotherapy with autologous stem cell transplantation rescue were indicated for patients with more aggressive disease, including women with more than three positive lymph nodes and those who were premenopausal or estrogen- and progesterone-receptor (ER and PgR) negative.
Radiotherapy was delivered to the breast at a dose of 50 Gy plus a boost of 10 Gy after the conclusion of chemotherapy or at least 30 days after surgery, when chemotherapy was not indicated.
Follow-Up
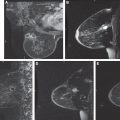
For the first 5 years after the surgery, the patients were seen at the clinic every 6 months by the clinical oncologist, breast surgeon, and/or plastic surgeon. In addition, the patients underwent a complete clinical checkup every year, which included blood examinations, chest radiography, liver ultrasonography, gynecologic ultrasonography (only in patients undergoing adjuvant therapy with tamoxifen), and mammography. Bone scans were performed only when indicated by blood examination or clinical symptoms. The patients were subsequently seen once a year, and all had annual mammography examinations. Our last follow-up was performed 18 years after the first surgical intervention. All of the patient charts were retrieved and updated in our database. We contacted patients by telephone interviews or through family members in the case of deceased individuals.
Statistical Analysis
The estimated crude cumulative incidence of tumor recurrence in the same breast after oncoplastic surgery, contralateral breast carcinomas, regional or distant metastasis, and other primary tumors was calculated according to a framework described by Marubini and Valsecchi. 10 The time to the occurrence of these events was computed from the date of surgery. The overall survival curves were obtained using the Kaplan-Meier method, and competing risk methods were used to assess the cumulative incidence of local recurrence and distant metastasis, depending on which event occurred first. Finally, the multivariate Cox proportional regression model was used to assess the effects of the independent prognostic value of the selected tumor and patient’s characteristics on the development of local recurrence, distant metastasis, or death. A statistical analysis was performed using SAS software. All tests were two sided.
Results
The average patient age was 50 years (range 31 to 71 years). Ninety-one patients (61.5%) were premenopausal, and 28 (18.9%) had grade I or grade II breast cancer in their family history. In 71 patients (48%) the tumor was in the right breast. A superolateral quadrant was involved in 47 patients (32%), a superomedial quadrant in 22 (15%), a union of superior quadrants in 17 (11%), an inferolateral quadrant in 17 (11%), an inferomedial quadrant in 16 (11%), a union of inferior quadrants in 15 (10%), a central quadrant in 15 (10%), a union of lateral quadrants in 2 (1%), and a union of medial quadrants in 1 (0.7%). In four patients (3%), we found tumors in two quadrants. One hundred thirty-seven patients (93%) had invasive tumors, and 11 (7%) had ductal carcinoma in situ (DCIS). The average size of the tumor determined in the pathologic analysis was 22 mm (range 3 to 100 mm), and 31 (21%) tumors were multifocal, with more than one lesion on the same quadrant. The mean weight of breast tissue from the breast containing the tumor was 198 g (range 20 to 2100 g).
Complete axillary dissections were performed in 129 patients (87%), and a sentinel node biopsy was done in 7 (5%); 12 (8%) did not receive any axillary treatment. Seventy-six patients (51%) had axillary metastasis. There were early complications (less than 2 months after surgery) in 16 patients (11%): wound infection in 7 (5%), hematoma in 4 (3%), partial nipple-areola necrosis in 2 (1%), breast seroma in 1 (0.7%), hypertrophic wound in 1 (0.7%), and partial wound dehiscence in 1 (0.7%). These complications did not delay the beginning of systemic and local adjuvant treatments.
An assessment of the excision margins showed complete excision of the tumor in 135 patients (91%), focally involved margins with DCIS in 8 patients (5.5%), and close margins (less than 2 mm) in 5 patients (3%). One patient with focally involved margins with DCIS underwent a total mastectomy and developed a local recurrence. Distant metastasis was subsequently detected, and she died 48 months after the first surgery. Other patients with focally involved margins received a boost in the tumor bed, similar to the patients with negative margins.
Characteristic | Cases (N = 148) | Characteristic | Cases (N = 148) |
Age (yr) | Hormone Receptor Status | ||
<40 | 18 | ER or PgR positive | 106 |
40–49 | 57 | ER and PgR negative | 35 |
50–59 | 50 | ER and PgR missing | 7 |
60–69 | 21 |
|
|
>70 | 2 |
|
|
Tumor Size (mm)* | Ki67 | ||
1–10 | 18 | 16 | 57 |
11–20 | 65 | >16 | 81 |
21–30 | 42 | Unknown | 10 |
>30 | 19 |
|
|
Grading | Axilla | ||
I | 34 | NX | 12 |
II | 60 | N0 | 60 |
III | 48 | N1mi | 8 |
Unknown | 6 | N1a | 44 |
|
| N2a | 13 |
|
| N3a | 11 |
Vascular Invasion | Adjuvant Chemotherapy* | ||
Yes | 54 | Yes | 89 |
No | 94 | No | 58 |
Multifocal Tumors | Adjuvant Hormone Therapy* | ||
Yes | 31 | Yes | 108 |
No | 117 | No | 39 |
Surgical Margins | Complementary Radiotherapy* | ||
Negative | 135 | Yes | 141 |
Positive | 8 |
|
|
Close (<2 mm) | 5 |
|
|
*Data were not available for all patients in these four categories.
All patients received some form of adjuvant systemic therapy. Seventy-one (48%) received the CMF regimen, 47 (32%) received the AC regimen, 31 (21%) followed the AC and CMF regimen, 2 (1%) had high-dose chemotherapy with autologous stem cell transplantation rescue as part of a study protocol, and 58 (39%) received no chemotherapy. Adjuvant hormone therapy with tamoxifen was indicated in 108 patients (73%). One hundred forty-one patients (95%) received adjuvant radiotherapy.
Local Recurrences and Distant Metastases
The median follow-up was 74 months (range 10 to 108 months), and only three patients (2%) of this group were lost to follow-up. Five patients developed an ipsilateral breast cancer recurrence (3%) in an average of 23 months (range 12 to 36 months) after the first surgery. Four patients had a recurrence in the tumor bed and one patient had a recurrence in the axilla. In the univariate analysis, the probability of local recurrence was significantly higher in the group of patients with tumors larger than 2 cm (p = 0.009), and in patients with Ki67 greater than 16 was closed up to significance (p = 0.06). Nineteen patients (13%) developed distant metastasis in an average time of 33 months (range 1 to 65 months) after the first surgery. The metastasis sites were: bone (13), liver (10), lung (7), brain (5), supraclavicular area (5), internal mammary chain (2), and skin (1). The risk of distant metastasis was significantly higher in the group of patients with tumors larger than 2 cm (p <0.0001), Ki67 greater than 16 (p = 0.007), and histologic grading G2 and G3 (p = 0.029).
The hazard ratio (HR), 95% confidence intervals (CI), and p value were obtained from the multivariate Cox proportional hazards regression model. (No association was found with the tumor grade, plurifocality, PVI, or Ki67.) NS, Not significant.
The sequence of events in 59 patients with pT2–3 tumors shows that 43 (73%) are free of disease, 5 (8%) had a local relapse (all developed distant metastases, and 4 died from the disease), and 11 (19%) developed distant metastases (6 died).
Other Events and the Contralateral Breast
Four patients underwent a quadrantectomy, four underwent a total mastectomy, and one had a modified radical mastectomy in the contralateral breast, because a second breast tumor was diagnosed in the follow-up.
Mortality
Eleven patients (7.4%) died of breast cancer at a median of 45 months after the first surgery. Ten patients had T2 tumors, 7 had a histologic grade of G3, 6 were ER/PgR negative, and 7 had positive axillary lymph nodes. (For the long-term oncologic results in oncoplastic surgery of the breast, see Table 34-3.) No events were registered in the DCIS group.
Stage | Patients | Relapse | Metastases | Death |
pTis | 11 | 0 | 0 | 0 |
pT1a–1b | 14 | 0 | 0 | 0 |
pT1c | 63 | 0 | 4 | 1 |
pT2–3 | 57 | 5 | 15 | 10 |
| pT | pN | Age | ER/PgR | Ki67 | Others |
First patient | 2 | 1a | 41 | + | 60 |
|
Second patient | 2 | 3a | 56 | ℒ | 33 |
|
Third patient | 2 | 1a | 39 | ℒ | 18 | PVI+ |
Fourth patient | 2 | 0 | 35 | ℒ | 70 | Margin+ |
Fifth patient | 2 | 1a | 33 | ℒ | 40 |
|
PVI, Peritumoral vascular invasion.
Three patients were lost to follow-up.
Related posts:
 32 Cancer Surveillance After Partial Breast Reconstruction
32 Cancer Surveillance After Partial Breast Reconstruction
 33 Complications and Outcomes After Immediate Partial Breast Reconstruction
33 Complications and Outcomes After Immediate Partial Breast Reconstruction
 4 Applied Anatomy and Breast Aesthetics: Definition and Assessment
4 Applied Anatomy and Breast Aesthetics: Definition and Assessment
 16 Reduction and Mastopexy Techniques With Parenchymal Autoaugmentation
16 Reduction and Mastopexy Techniques With Parenchymal Autoaugmentation
 28 Local Perforator Flaps in Oncoplastic Breast-Conserving Surgery: The Nottingham Experience
28 Local Perforator Flaps in Oncoplastic Breast-Conserving Surgery: The Nottingham Experience
 24 Classification and Analysis of the Breast-Conserving Therapy Deformity
24 Classification and Analysis of the Breast-Conserving Therapy Deformity
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


