4 Applied Anatomy and Breast Aesthetics: Definition and Assessment
As surgical approaches to breast surgery continue to evolve and improve, some aspects remain the same, such as breast anatomy and our understanding of the qualities that make an aesthetically pleasing breast form. It is crucial to have a thorough understanding of breast anatomy and an aesthetic ideal or goal when performing breast surgery. In this chapter we discuss basic breast anatomy and the factors that define the aesthetic ideal of breast form. These concepts should be reviewed and applied to every surgical procedure performed on the breast.
Breast Embryology and Development
The breast is a specialized gland that originates from the ectoderm. The fetal breast begins to form during the sixth week of gestation, with the growth of a milk ridge extending from the axilla to the groin. By the eighth to tenth week of development, the epithelium in the pectoral region begins to differentiate into breast tissue.
Supernumerary breasts and nipples can be found anywhere along the milk ridge and may be capable of both lactation and cancer formation.
After birth, an infant’s breast may secrete milk for a short time because of high levels of circulating maternal hormones. The breast tissue becomes dormant until puberty, which normally occurs between the ages of 9 and 14. At this time, a breast bud develops just beneath the nipple and may be firm and tender. During puberty, the breast bud begins to grow in response to increased levels of circulating hormones. Lobular units develop, and ducts elongate and branch. Breast development usually concludes when the individual reaches her maximum vertical height. The postpubertal breast continues to change according to cyclic variations in the circulating hormones.
Congenital breast asymmetry may occur. If cancer is diagnosed in the larger breast, then symmetry may be improved after breast-conserving therapy (BCT), as long as the breast shape is preserved.
Breast Composition
The breast comprises many subunits: skin, glandular parenchyma, fat, blood vessels, nerves, lymphatics, and connective tissue. Each of these breast subunits must be considered when closing or reconstructing partial mastectomy defects to avoid potential contour irregularities and deformities.
The breast is also closely associated with the underlying muscle and chest wall, which contribute to the overall form, shape, and appearance of the breast. The breast’s boundaries extend from the clavicle to the inframammary crease in the craniocaudal direction and from the midsternum to the lateral breast fold in the mediolateral direction. The breast’s axillary tail extends through the axillary fascia into the axillary tissue. Fascial attachments anchor the breast to the chest wall and skin.
The Skin
The breast skin is a very important component of breast anatomy. The quality, elasticity, and thickness of the skin significantly influence the overall appearance of the breast. Differences in skin types alter outcomes in breast surgery. For instance, patients with thin, poorly elastic skin develop recurrent ptosis after mastopexy at a much faster pace than those with thick, more elastic skin.
The patient’s age, hormone levels, and weight fluctuations—as well as gravity and external factors such as radiotherapy—can significantly alter the quality of the breast skin. If the skin becomes overstretched, striae and tears can occur. If the skin is thin and stretched too much during breast surgery, scars may widen. The thickness of the dermis varies in different regions of the breast. The dermis is very thin in the central portion of the breast around the nipple and areola. This contributes to the protrusion of glandular tissue through this region, resulting in deformities such as tubular or tuberous breasts. The dermis becomes much thicker and adheres more to the epithelium near the inframammary crease, which is why it is more difficult to deepithelialize skin in this region. Breast remodeling should minimize the use of skin for shaping.
The surgeon must thoroughly understand the blood and nerve supply to the breast skin to prevent ischemia or numbness after breast surgery. To minimize morbidity, the surgeon must also be aware of previous incisions when planning breast surgery. The primary blood supply is from the subdermal plexus, which communicates with underlying parenchymal and chest wall perforators. Innervation of the breast skin is segmental and follows typical dermatomal patterns. Breast skin innervation comes primarily from the anteromedial and anterolateral branches off the intercostal nerves at the level of T3-5. Upper breast sensation also derives from branches emanating from the lower cervical plexus.
Skin replacement is often required to preserve shape, especially in women with smaller breasts who undergo quadrantectomy-type resections.
Skin replacement is intentionally overcorrected in anticipation of fibrosis. To minimize skin necrosis, skin flaps should not be extensively undermined. The flap should be designed and inset in a manner that reconstructs aesthetic units to minimize the patchwork appearance.
The Glandular Parenchyma
The majority of the breast volume consists of glandular parenchyma and fat. The proportions of each of these components vary from person to person. Factors such as genetics, hormones, weight fluctuations, age, and the percentage of body fat influence this balance.
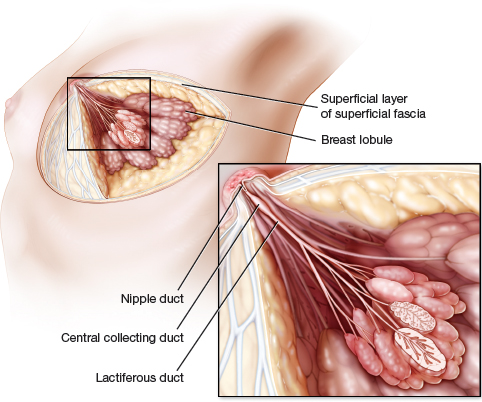
The glandular component of breast parenchyma is specialized for producing and secreting milk. It consists of an intricate system of breast lobules that are distributed radially throughout the breast tissue. The functional subunits of each breast lobule are hundreds of secretory acini that empty their secretions into interlobular ducts. The interlobular ducts then drain into lactiferous ducts, which carry secretions to central collecting ducts located below the nipple. These secretions exit the nipple through nipple ducts.
This ductal system allows bacteria to colonize the breast. Staphylococcus epidermidis may be cultured in breast tissue and can increase the risk of a postoperative wound infection.
The Fat
The fat content affects the shape, contour, softness, and texture of the breast. Fattier breasts are generally softer and more supple, but they tend to develop ptosis more quickly. In addition, fatty breasts are more likely to develop fat necrosis. Densely glandular breasts tend to be firm and more irregular but usually maintain their shape longer. After menopause the content of breast fat increases and the amount of glandular tissue decreases. Exogenous hormone administration slows this process.
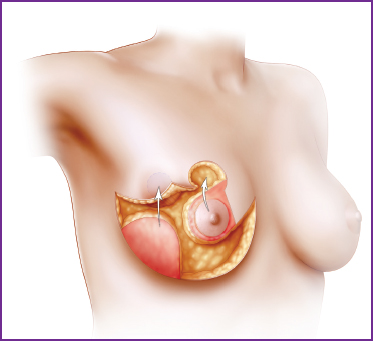
The Connective Tissue
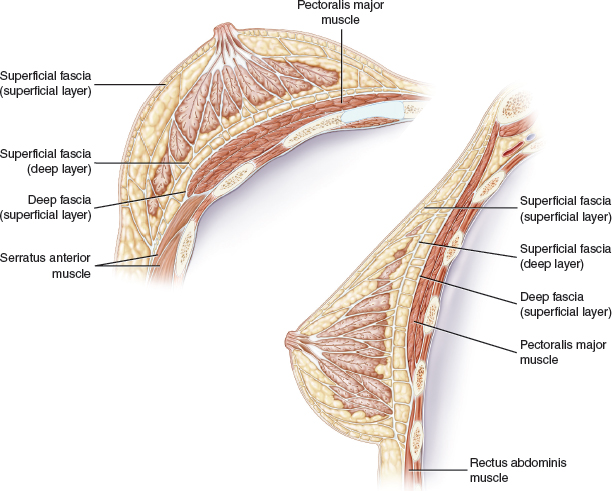
Within the breast, multiple supporting layers of connective tissue help to maintain the form, shape, and appearance. The fascia is divided into superficial and deep layers. The superficial layer is further subdivided into superficial and deep layers. The superficial layer of the superficial fascia is located just beneath the dermis; it is the outermost covering of the breast parenchyma. Depending on the individual, there may be a thin layer of subcutaneous fat between the dermis and the superficial fascia. This is the location of the subdermal plexus of blood vessels, which supplies blood to the skin.
The deep layer of the superficial fascia is located on the posterior surface of the breast and separates the parenchyma from the underlying deep fascia covering the chest muscles. A thin layer of loose areolar connective tissue separates these two fascial planes. The deep fascia covers the pectoralis major, serratus anterior, external oblique, and upper portion of the rectus abdominis muscles beneath the breast.
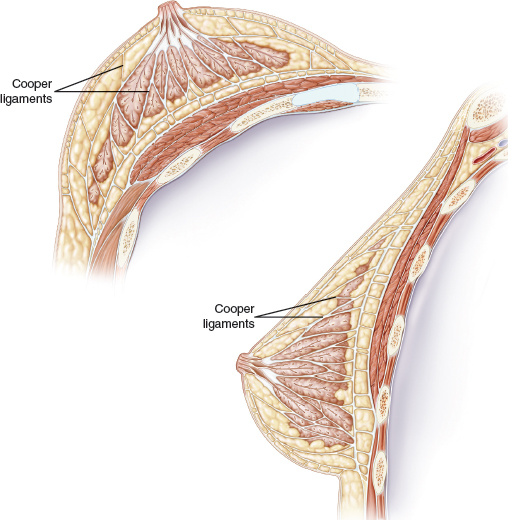
The suspensory ligaments of Cooper contribute to breast form, shape, and elasticity. These connective tissue bands attach to the deep fascia and pass through both layers of the superficial fascia and the breast parenchyma before attaching to the dermis. Cooper ligaments stretch with weight fluctuations, aging, and pregnancy, causing elongation and decreased elasticity and contributing to breast ptosis. Appreciating the ligamentous structures of the breast is required to accurately reposition the breast subunits when local parenchymal flaps are used.
The Muscles
It is important to understand the musculature of the anterolateral chest wall because of its shared blood, nerve, and lymphatic supply with the breasts. These muscles also play a prominent role in breast reconstruction and aesthetic breast surgery. Additionally, their absence or partial absence, as in Poland’s syndrome, has a profound impact on the appearance of the breast.
The major muscles of interest are the pectoralis major and minor muscles, which lie beneath the upper central and lower medial portions of the breast. The lower lateral breast tissue covers the serratus anterior, the upper portion of the rectus abdominis, and the upper external oblique muscles.
The Blood Supply
The blood supply to the breast comes from numerous sources and allows many different approaches to breast surgery. Multiple factors can influence how robust each of these sources of inflow may be. The patient’s age, endocrine activity, overall health, and microcirculation alter the inflow. After menopause, blood flow to the breast decreases. Likewise, the quality of the microcirculation is altered by conditions such as diabetes, atherosclerotic disease, collagen vascular disease, smoking, and radiotherapy. Because of the substantial collateralization of arterial flow within breast tissue, survival of the entire breast is possible with only a fraction of the inflow.
It is very important to understand the intimate relationships among the blood supply to the chest wall, the breast parenchyma, and the overlying breast skin when planning reconstructive and aesthetic breast surgical procedures. In addition, it is critical to appreciate the blood supply when raising large parenchymal flaps and to maximize the blood supply to prevent ischemia in breast surgery. Suture plication should be minimized to prevent tissue ischemia.
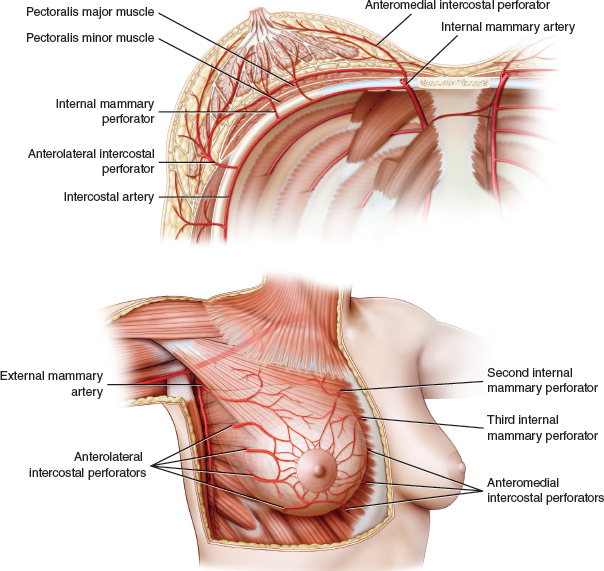
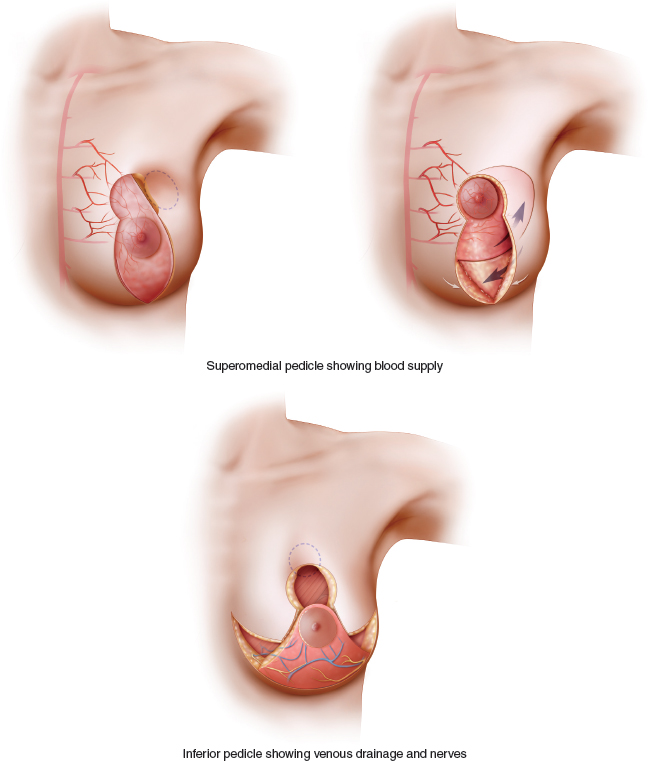
The major sources of inflow to the breast, from medial to lateral, are the internal mammary segmental perforators, the intercostal perforators, the thoracoacromial perforators, and the external mammary artery. The internal mammary perforators penetrate the medial intercostal spaces between the second and sixth ribs. They supply the pectoralis major muscle, the breast tissue, and the overlying skin. The second and third perforators are the largest, and they supply the primary blood flow to the upper medial breast. These provide the dominant blood supply to the pedicle in the superomedial reduction mammaplasty technique.
The intercostal perforators exit from the intercostal arteries in the third through sixth intercostal spaces. They penetrate the chest wall at the lateral margin of the pectoralis major muscle, pass through the serratus anterior muscle, and enter the breast parenchyma. These perforators supply the lateral breast tissue and skin, and they send branches to the latissimus dorsi muscle.
Another group of intercostal perforators (anteromedial) supplies the central and lower medial aspect of the breast parenchyma. These perforators penetrate the chest wall in the fourth through sixth intercostal spaces. They are the primary source of blood flow to the pedicle in the inferior central mound reduction mammaplasty technique. The anteromedial and anterolateral intercostal perforators extend to the NAC and are major contributors to vascularization of the nipple.
The thoracoacromial artery enters the pectoralis major muscle and supplies perforators to the overlying upper, central, and lower breast tissue. During augmentation mammaplasty, these perforators are divided in the subglandular dissection but are preserved in the submuscular dissection. The external mammary artery enters the upper lateral breast after exiting the axillary artery. This artery may be as large as 2 to 3 mm in diameter and may provide nourishment to the entire breast.
Unnecessary undermining on the breast periphery should be minimized, because it could jeopardize the use of perforators from the intercostal muscles that could be used as perforator flaps. This could also compromise breast perfusion, resulting in skin and fat necrosis.
Related posts:
 6 Breast-Conserving Therapy: Decision-Making and Anticipating the Unfavorable Aesthetic and Functional Result
6 Breast-Conserving Therapy: Decision-Making and Anticipating the Unfavorable Aesthetic and Functional Result
 10 Breast Radiotherapy in Oncoplastic Surgery
10 Breast Radiotherapy in Oncoplastic Surgery
 11 Indications and Benefits of Oncoplastic Breast Surgery
11 Indications and Benefits of Oncoplastic Breast Surgery
 9 Improving the Quadrantectomy Defect
9 Improving the Quadrantectomy Defect
 14 Psychosocial Aspects of Oncoplastic Breast Conservation
14 Psychosocial Aspects of Oncoplastic Breast Conservation
 13 Timing of the Oncoplastic Reconstruction: Immediate, Delayed, and Delayed-Immediate
13 Timing of the Oncoplastic Reconstruction: Immediate, Delayed, and Delayed-Immediate
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


