13 Timing of the Oncoplastic Reconstruction: Immediate, Delayed, and Delayed-Immediate
Oncoplastic reconstruction may begin at the time of BCT/BCT (immediate), weeks (delayed-immediate), or months to years afterward (delayed). 1 Not every oncologic surgeon planning to perform BCT intends to use any type of oncoplastic procedure, and some patients are satisfied with the use of external breast prostheses worn under clothing. However, with immediate reconstruction, the surgical process is smooth, because both BCT and reconstruction can be completed in one operative setting. Additionally, the emotional benefit for the patient of having begun reconstruction at the time of the oncologic procedure may decrease the impact of the loss. Conversely, the surgical time can be lengthened and potential complications such skin necrosis, dehiscence, or infection can unfavorably affect the outcome. Although the immediate approach permits wider excision of the tumor, 2 – 5 the whole procedure can be compromised by positive histologic margins. In addition, some patients are so distressed by their cancer diagnosis that they are not capable of significantly participating in reconstructive considerations, and delayed reconstruction will defer the need to make a decision about it. On the other hand, delayed reconstructions can be technically difficult, since these patients have scarred breast tissue as a result of previous procedures and fibrosis from radiotherapy. 1 , 2 , 5 – 7
Despite these arguments for and against, surgical planning should include breast volume, tumor location, the extent of glandular tissue resected, and chiefly addressing individual reconstructive requirements, enabling each patient to receive an individual, custom reconstruction. Evaluation of BCT reconstruction must subsequently consider these important points and, only then should the proper technique at an appropriate time be chosen. In addition, an in-depth dialogue concerning alternatives for BCT reconstruction should be undertaken with the patient and her family, including the risks and positive aspects of the time of approach of reconstruction.
Immediate Reconstruction
The immediate application of oncoplastic techniques to BCT is an expected reaction to the realization that aesthetic outcome following BCT and radiotherapy is occasionally disappointing. 8 The major advantage of the immediate approach is that BCT and reconstruction can be achieved in a one-stage surgery and the patient does not have to cope with a deformity following the operation. Because there is no glandular and skin scar tissue, breast reshaping is easier, and the cosmetic results are improved. 1 , 3
When the potential for a deformity exists preoperatively, immediate reconstruction is preferred; however, it should not jeopardize the oncologic outcome or delay radiotherapy.

These two patients have poor aesthetic outcomes following conservative breast surgery and radiotherapy without reconstruction.
Patient Example
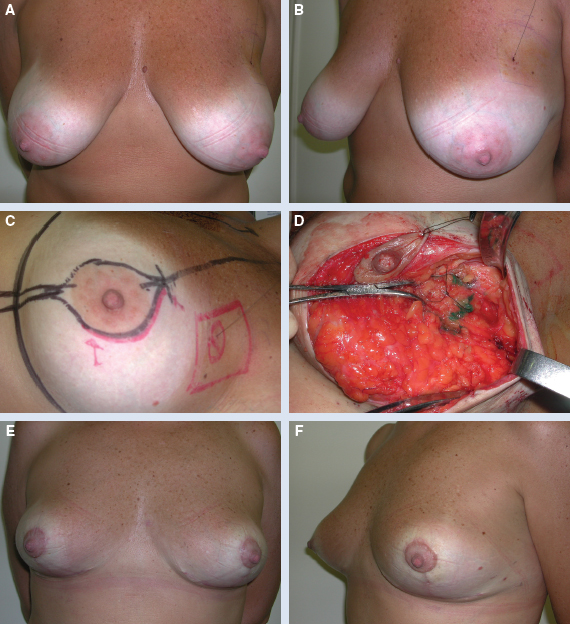
This 48-year-old patient had a 1.9 cm invasive ductal carcinoma of the left breast (A and B). She underwent a left superolateral quadrantectomy and sentinel lymph node biopsy, immediately followed by a bilateral reduction mammaplasty reconstruction. A total of 125 g was removed from the left breast and 145 g from the right breast (C and D). She is shown 8 months postoperatively with a very good outcome after radiotherapy (E and F).
Thus it is advocated that the treatment of choice should be preventive by preoperative planning and immediate breast repair before adjuvant radiotherapy. 1 – 3 , 8 Papp et al, 9 in a comparative series of 40 immediate and delayed reconstructions, observed that the cosmetic results showed a higher success rate in the immediate repair group compared with the delayed reconstruction patients, of which 16% had poor ratings. Similarly, Kronowitz et al 3 observed that delayed reconstruction usually required the use of autologous tissue to provide additional blood supply to assist with healing within the irradiated operative field. Despite the fact that radiotherapy has a negative impact on the cosmetic result, some authors suggest that the incidence of related complications varies, depending on the radiation technique used. 2 , 6 The total radiation dose, the use of radiation boost, and the number of radiation fields are important related risk factors. 10 , 11 Beadle et al 10 did not observe radiotherapy complications in patients without radiation boost compared with 22% of complications in those treated with boost therapy. Correspondingly, Harris et al 11 observed that increasing the external irradiation dose (more than 60 Gy) was associated with a high incidence of skin fibrosis. In our previous studies, 12 – 15 the maximum radiation dose used was 50 Gy to the remaining breast tissue and an additional boost of 10 Gy to the tumor site. In these studies, the majority of complications occurred in the initial postoperative period.
Outcomes
In our previous experience comparing the outcome following immediate and delayed reconstruction, we performed a retrospective review to compare complications, length of hospital stay, the need for revision surgeries, and satisfaction. 16 In this series, the immediate approach was more advantageous because of the benefits of less psychological impairment. In addition, most of the complications were observed in the reconstructed breast and occurred in the initial postoperative period. One might surmise that previous oncologic manipulations and axillary dissection may be involved. However, there were no significant differences between patients who underwent axillary dissection and the sentinel lymph node biopsy in terms of complications. A total of 144 patients were followed for a mean of 47 months. Of the 106 patients in the immediate group, complications occurred in 24 (22.6%), skin necrosis was observed in 7.5%, fat necrosis in 5.6%, and 6.6% of patients developed local recurrence. The mean period of hospitalization was 1.89 days. Of the 38 patients in the delayed group, complications occurred in 12 (31.5%), skin necrosis was observed in 7 (18.4%), fat necrosis in 4 (10.5%), and 5.2% of patients developed local recurrence. The mean period of hospitalization was 1.35 days. An increased length of hospital stay greater than 1 day (p <0.001) and the number of revision surgeries (p <0.043) were associated with the timing of the reconstruction. In univariate analysis, no difference between groups was found with respect to the incidence of complications (p <0.275); however, after adjusting for other risk factors, the probability of complications tends to be higher for the delayed group (OR = 2.65; 95% confidence interval = 1.01 to 7.00; p = 0.049). In a recent series by Egro et al 17 evaluating the timing of the reduction techniques, the complication rate and reoperation rate were significantly lower in the immediate group compared with the delayed group.
Oncologic Advantages
Immediate reconstruction can provide beneficial oncologic advantages in some groups of patients. Some studies observed that patients with macromastia present more radiation-related complications than patients with normal volume breasts. 10 , 11 Thus immediate breast reduction can increase the eligibility of large-breasted patients for BCT, since it can reduce the difficulty of providing radiotherapy to the remaining breast tissues. 6 , 10 , 11 , 18 – 20 Brierley et al 19 evaluated the correlation between late radiation reaction and brassiere size and demonstrated that late radiation fibrosis occured 36% of the time in patients with larger breasts, compared with 3.6% for smaller breasts. Similarly, Gray et al 20 found that there was more retraction and asymmetry in the large-breasted versus the small-breasted group. Therefore it is common knowledge that the reduced size of the breast allows for more homogeneous delivery of radiation dose at lower levels, reducing late radiation complications. 18 – 20
Margin Issues
Another important factor in immediate reconstruction is the possibility of accomplishing a widely negative resection margin around the tumor. In fact, the immediate approach allows wider local tumor excision, potentially reducing the incidence of margin involvement and the development of local recurrence. 1 , 3 – 5
Patient Example

This 61-year-old patient was diagnosed with a 3.5 cm invasive ductal carcinoma of the left breast (A and B). The patient underwent a left central-inferior quadrantectomy and total axillary dissection, immediately followed by a bilateral reduction mammaplasty reconstruction. A total of 225 g was removed from the left breast and 235 g from the right breast (C and D). She is shown 1 year postoperatively with a good outcome after radiotherapy (E and F).
Kaur et al 4 compared patients who underwent oncoplastic procedures and conventional quadrantectomy in terms of the volume of tissue excised and surgical margins. The immediate oncoplastic approaches permitted larger resections, with a superior mean volume of the specimen and negative margins. Losken et al 7 demonstrated a significantly lower positive margin rate in a series of oncoplastic reduction patients compared with patients who underwent BCT alone, and this was also noted in a recent meta-analysis. The positive margin rate was 12.2% in the oncoplastic group and 20.6% in the BCT-alone group (p <0.001). The translation of this to a long-term recurrence rate is unknown. Kronowitz et al 3 reported a rate of local recurrence of 5% with breast reduction, compared with 13% for patients treated with the flap technique, in which no additional breast tissue is usually removed.
When immediate reconstruction is indicated, every attempt should be made to minimize the possibility of positive margins.
Although immediate BCT reconstruction does not represent a problem in routine postoperative cancer surveillance, 5 , 7 , 12 – 15 it may lead to difficulty in establishing the location of a positive surgical margin postoperatively. Another important concern is postoperative scarring, which may mimic or obscure malignancy on mammography. 6 , 14 , 15 Although these changes are well understood, and discrimination between tumor recurrence and fat necrosis can usually be differentiated in major cancer centers, we advocate careful surveillance and biopsy to elucidate a local recurrence. 21 When a breast-reduction technique is performed, it is important to use one that employs safe flaps and has a low risk of fat necrosis. 15
Scar tissue may mimic or obscure malignancy, and the appearance of a new mass can be similar to a normal scar on mammography.
All reconstructive techniques that involve rearrangement of glandular tissue make reexcision difficult and may jeopardize the oncologic treatment in cases in which close or positive margins are observed. 13 – 15 This fact could make it difficult to locate the residual tumor and to perform margin reexcision. Additionally, intraoperative evaluation of surgical margins can present some limitations and as with any other test, there is an inherent false-positive and false-negative rate. 21 Rietjens et al, 5 in a recent study from a Milan group, reported an 8% positive or close margin involvement, which is lower than the 10% observed in the NSABP B-06 trial. Conversely, Kronowitz et al 3 revealed that postoperative margins were positive in 15.7% of patients who underwent partial mastectomy without reconstruction. The authors emphasized that these patients had defect sizes four times smaller than the defects in the patients who underwent reconstruction. Larger defects in patients who undergo immediate reconstruction usually correlated with a lower incidence of positive postoperative tumor margins in this study.
If there are concerns about the margin status, the reconstruction should be deferred until final negative margins are obtained.
Related posts:
 6 Breast-Conserving Therapy: Decision-Making and Anticipating the Unfavorable Aesthetic and Functional Result
6 Breast-Conserving Therapy: Decision-Making and Anticipating the Unfavorable Aesthetic and Functional Result
 10 Breast Radiotherapy in Oncoplastic Surgery
10 Breast Radiotherapy in Oncoplastic Surgery
 11 Indications and Benefits of Oncoplastic Breast Surgery
11 Indications and Benefits of Oncoplastic Breast Surgery
 9 Improving the Quadrantectomy Defect
9 Improving the Quadrantectomy Defect
 4 Applied Anatomy and Breast Aesthetics: Definition and Assessment
4 Applied Anatomy and Breast Aesthetics: Definition and Assessment
 14 Psychosocial Aspects of Oncoplastic Breast Conservation
14 Psychosocial Aspects of Oncoplastic Breast Conservation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


