33 Philosophy and Principles of Rhinoplasty
Introduction
Rhinoplasty is widely regarded as the most challenging operation in facial plastic surgery. Much of the difficulty lies in understanding the threedimensional configuration of the osseocartilaginous framework and its translation into external contour. While rhinoplasty is a continually evolving operation, the underlying philosophy and principles have not changed much over recent years. However, a better understanding of nasal analysis, interplay of anatomy and function, and longterm postoperative healing have led to refinement of surgical techniques. All these factors have contributed to improved longterm aesthetic and functional results.
In the advent years of rhinoplasty, most techniques were reductive, focusing on dorsal hump excision and nasal tip refinement. Functional aspects, particularly longterm, were either not known or simply ignored. Endonasal approaches were commonly used, leading to less than ideal exposures with imprecise and often uneven structural resections. Compromised outcomes were hidden behind camouflaging effects of soft tissue edema. Noses began to appear pinched and scooped over time, leading to nasal obstruction.
In recent years, the pendulum has swung toward an emphasis on both: function and form. Finding the right balance between the two is now a priority of the contemporary rhinoplasty surgeon. More emphasis is placed on preservation of key anatomical structures to highlight higher nasal dorsums with complementary tip projection. 1 The increased popularity of external rhinoplasty approaches has allowed surgeons to accurately assess the patients’ anatomical problems and precisely modify the underlying structural framework. Some may argue, however, that the increased exposure afforded by the external approach allows the surgeon to make more radical alterations to the nose, which can lead to more complications. 2
Inherent histologic tissue changes occur with aging, while constant external forces act on the nose’s structural support system; with each inspired breath, the nose tends to collapse. It is the role of the skeletal framework to prevent the overlying skin–soft tissue envelope (SSTE) from collapsing. In contrast to the common belief that noses enlarge with aging, they tend to become narrower and more pinched over time. The nasal appearance 1 week postoperatively may differ greatly from the appearance at 6 months, 1 year, and thereafter. While the surgeon controls the operative intervention, it is equally important to develop skills in manipulating and controlling dynamics of postoperative healing. The operation itself should be considered the first, and not the last, intervention in altering someone’s nasal shape and function. Maintaining and establishing structural support of the nose is hence critical, withstanding the aforementioned forces that may otherwise lead to suboptimal functional and aesthetic results.
The idiom that no two noses are alike certainly holds true in rhinoplasty. Even among identical twins, variations in nasal anatomy have been observed, likely due to a variety of congenital and environmental effects. It follows that every rhinoplasty presents the surgeon with a wide array of nasal anatomy, contours, and proportions, necessitating a series of organized and interrelated surgical maneuvers tailored to each patient’s needs. The aesthetic judgment of the surgeon, guided by the patient’s wishes, determines the surgical plan. No single procedure or technique will suffice to adequately reconstruct every nose. Many years of experience are required to critically observe, analyze, modify, and perfect surgical results. With the increased popularity of external rhinoplasty techniques, less experienced surgeons may be able to perform more precise maneuvers through improved visualization. Inappropriate and optimistic attempts to create changes greater than the tissues will permit may yield complications from overaggressive resection of supporting structures and should be avoided. Reductive techniques that were popular decades ago have now been replaced by more augmentative, structurally preserving techniques. Proper preoperative and intraoperative analysis with identification of correctable deformities and recognition of surgical limitations is critical to achieve consistently successful outcomes.
Nomenclature
Rhinoplasty stems from the Greek term rhis (nose) and plassein (to shape). It may be defined as any operative procedure that corrects and reconstructs the form, restores the function, and aesthetically enhances the nose. Primary rhinoplasty refers to an operation in a previously unoperated nose, whereas the term secondary should be reserved for patients who had at least one prior rhinoplasty by another surgeon. The term revision rhinoplasty is frequently used interchangeably with secondary, even though revision most accurately describes a secondary operation performed by the same (not different) surgeon who performed the previous operation.
The terms incision, approach, and technique also require differentiation. An incision is a surgically created cut to gain access to the underlying nasal skeletal framework. The commonly used rhinoplasty incisions are transcolumellar, marginal, transcartilaginous (cartilage-splitting), intercartilaginous, and rim incisions. An approach describes the specific anatomical dissection that provides exposure to the skeletal structures. The commonly used approaches are either endonasal (closed) or external (open). Endonasal approaches may be further categorized as either delivery or nondelivery, the latter of which may be performed either via a transcartilaginous (cartilage-splitting) or retrograde approach. The term technique describes any maneuver, specific method of procedure, or details of a given operation (e.g., excision, reorientation, or reconstruction of the lower lateral cartilages to produce a predicted change in size, shape, projection, rotation, and definition of the nasal tip).
Nasal Anatomy
The nose may be separated into several anatomical components, which include the SSTE, the bony pyramid or bony vault (nasal bones, osseous septum, and ascending processes of the maxilla), the cartilaginous pyramid or middle vault (upper lateral cartilages and cartilaginous septum), and the nasal tip (lower lateral cartilages). 3 The nasal tip consists of the tip lobule, alar sidewalls, infratip lobule, and columella.
The rich arterial blood supply to the nose is derived from branches of the external carotid system, mainly the facial and superior labial arteries. 4 The arteries are accompanied by corresponding veins and lymphatics, all of which run within the superficial musculoaponeurotic system (SMAS). Elevating the SSTE off the underlying nasal skeleton should be performed deep to the SMAS during rhinoplasty to preserve maximal blood supply, minimizing the risk of intraoperative bleeding and postoperative ischemia with possible tissue necrosis. Staying in the proper plane of dissection is particularly important in revision and secondary cases, where the baseline blood supply may already be compromised.
Patient Evaluation
Patient Interview
During the initial consultation, the surgeon should inquire about the patient’s goals, evaluate if the patient has realistic expectations, and determine if the patient is a good candidate for surgery overall. The patient needs to understand the possibilities and limitations of rhinoplasty. Establishing a trustworthy patient–physician relationship that allows both parties to communicate realistic expectations is an important goal for the consultation. Photography and computer imaging are helpful tools to assist in effective communication.
In cases of secondary rhinoplasty, the surgeon should also review prior operative notes, surgical worksheets, and old photographs, with the understanding that prior operative notes may contain incomplete or erroneous information. 5 Proper preoperative counseling for secondary cases requires knowledge of available grafting material, and whether alloplastic implants or injectable fillers are present.
Independent of whether a primary or secondary operation is planned, the surgeon may be able to identify a small subset of patients who may never be satisfied with their outcome. Some of these patients may demonstrate differing degrees of body dysmorphic disorder (BDD). 6 Caution should be exercised when planning to proceed with surgery in such patients; when in doubt, it is best not to proceed with the operation. Once, however, the surgeon understands the patient’s goals and the patient has realistic expectations about the procedure, surgery may ensue. 7
Physical Exam
External Exam
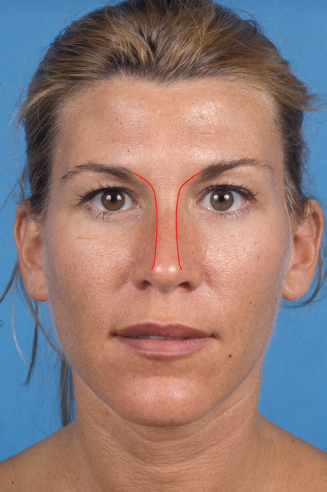
A thorough and systematic physical exam with accurate diagnosis is critical to a successful operation. The general shape of the face, the horizontal thirds, and the vertical fifths should be analyzed. Global assessment of nasal deformities in context to the remaining facial features often shows one or two readily noticeable problem areas. These deformities should be prioritized during surgery, as modification of any nasal structure influences the appearance of neighboring structures. 7 The patient’s ethnicity, the surgeon’s sense of aesthetics, and the surgeon’s ability to create a desired shape are other factors to be taken into consideration. Furthermore, body stature plays an important role as well. A patient of short stature may tolerate a more rotated nose better than a tall patient. Similarly, the degree of appropriate nasal projection depends on the projection and shape of the chin and mandible. For instance, an overprojected nose may not appear as unsightly in a patient with a strong chin and mandible as in a patient with a weaker chin and mandible. Conversely, an adequately projected nose may appear overprojected in a patient with an underprojected or retrognathic chin ( Fig. 33.1 ).

The thickness and sebaceous quality of the skin must be examined. Moderate skin thickness is optimal as it conforms reasonably well to the underlying skeletal framework thereby giving a desired shape to the nose and simultaneously provides a satisfactory cushion to hide small, undesired contour irregularities. Thin skin, however, is very problematic, as many irregularities in the underlying structure will show with time. Extremely thin skin is often pale and freckled, and must be recognized preoperatively for its inherent limitations. While thin skin may be optimal for obtaining definition, its limited subcutaneous tissue provides essentially no cushion to camouflage possible contour irregularities. Thin skin has more of a tendency to contract postoperatively, which may contribute further to show imperfections. If a thinskinned nose is downsized, the skin may take on a thicker character as long as extreme contraction does not occur. Working with thin skin hence requires near-perfect surgery to achieve the desired outcome. In contrast, thick skin conceals minor irregularities but can exhibit prolonged postoperative edema. Furthermore, it possesses memory of its own. With thick-skinned noses, the surgeon must resist the temptation to aggressively reduce the underlying cartilages in order to affect a contour change in overlying soft tissues. Such maneuvers tend to weaken nasal skeletal support, which may ultimately buckle and collapse under the forces of scar contracture. The memory of thick skin may prevent skin re-draping altogether, leaving a dead space with ensuing soft tissue pollybeak formation. For patients with thick skin, it is preferable to maintain or increase tip projection to stretch the SSTE to attain more definition. On the other hand, deprojecting a thick-skinned nose is a very challenging task and must be done judiciously to avoid undesirable skin redundancy and a pollybeak ( Fig. 33.2 ).

Evaluation of skin thickness is performed by close inspection and digital palpation. Gentle pinching of the SSTE allows the surgeon to analyze how it glides over the nasal skeleton. In cases of secondary rhinoplasty, lack of SSTE elasticity and mobility may reflect severe scarring and contracture, indicating an added risk during dissection at the time of secondary surgery. Shortage of vestibular lining at the marginal incision might require addition of lining, using auricular composite skin/cartilage grafts to allow for a tensionfree closure. Should there be any doubt regarding the integrity of the SSTE, secondary surgery should be delayed. Staged repair of the SSTE using skin grafts, local, or regional flaps should be considered prior to any structural nasal surgery.
Externally, the upper, middle, and lower thirds are assessed for deviation, irregularities, asymmetries, and width. External warning signs for the existence or development of nasal obstruction include a thin SSTE, a narrow middle vault, short nasal bones, a prominent supra-alar crease, supra-alar pinching, thin lateral nasal walls, dynamic lateral wall collapse, and narrow nostrils ( Fig. 33.3 ). Palpation of the nose is important in assessing the nasal skeleton for shape, strength, and symmetry. The resistance and recoil of the nasal tip to digital pressure provides important information about tip support. A nose that lacks tip support probably has weak lower lateral cartilages (LLCs) that will not tolerate much loss of support through aggressive tissue excision. The addition of supporting struts in such cases helps prevent postoperative loss of tip support. On the other hand, noses with vigorous tip recoil to palpation tolerate surgical manipulation of the LLCs much better without a significant loss of tip support. Palpation of the LLCs with two fingers may provide the surgeon with important information about the size, shape, and strength of the LLCs. 7

Furthermore, the caudal septum and columella should be palpated between the thumb and index finger to gain information about the relationship between those two structures. The caudal septum may be deviated or twisted, or the quadrangular cartilage may be overdeveloped, pushing the medial crura and columella inferiorly, creating the appearance of a hanging columella. The medial crura may be set back on an overly long caudal septum in a tonguein-groove fashion with or without excising a small strip of caudal septal cartilage to address the hanging columella. 8 In the vast majority of cases, however, the caudal septum does not require excision but rather should be preserved to avoid compromised tip support. In fact, a caudal septal extension graft (CSEG) is frequently placed to allow for medial crural setback. Knowledge of the width and length of the medial crura and columella is important, as this anatomical complex provides structural support. Short medial crura usually require placement of a columellar strut or caudal septal extension graft to provide tip support and thereby prevent postoperative loss of tip projection ( Fig. 33.4 ). 9

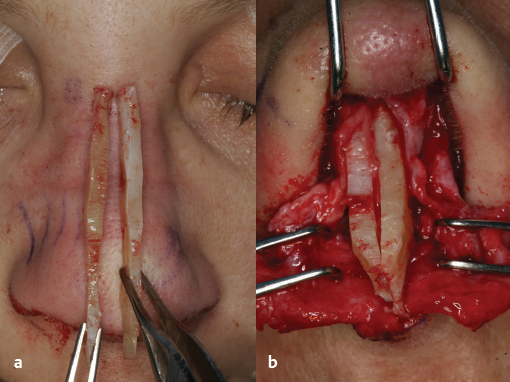
The length and strength of the upper lateral cartilages (ULCs) should be compared to the nasal bone lengths. Patients with short nasal bones tend to have less support at the internal nasal valve region (angle defined by the nasal septum, caudal margin of the ULCs, head of the inferior turbinate, and floor of the nose) because the associated longer ULCs tend toward inward collapse with negative inspiratory forces. This scenario particularly holds true in cases of dorsal hump reduction, leaving the caudal margin of the ULCs with even less support. Spreader graft placement between the dorsal septum and upper lateral cartilages is crucial in reestablishing and reinforcing middle vault support. Without such support, the middle vault may appear narrowed and lead to an inverted-V deformity from the inferomedial displacement of the ULCs ( Fig. 33.5 ). 9

On frontal view, nasal symmetry and width of each vertical third are assessed. The brow-tip aesthetic line, which should be a subtle hourglassshaped curvilinear line between the medial brow and nasal tip, should follow a pattern of relative width at the bony vault, slight narrowing at the middle vault, and relative width again at the tip ( Fig. 33.6 ). It provides important information about contour irregularities. 10 Exaggeration of the curvature may indicate excessive width at the bony vault or tip, or it may indicate middle vault pinching. The transition from the columella to alar margins should be a gentle “gull in flight” configuration ( Fig. 33.7 ). An excessively low “body” may indicate either a hanging columella or retracted alae. The size and shape of the alae and alar base should also be examined, with emphasis on how the alar width and flare may be altered through increasing or decreasing tip projection. In some cases, alar base excisions may still be necessary to provide harmony with the remainder of the nose.
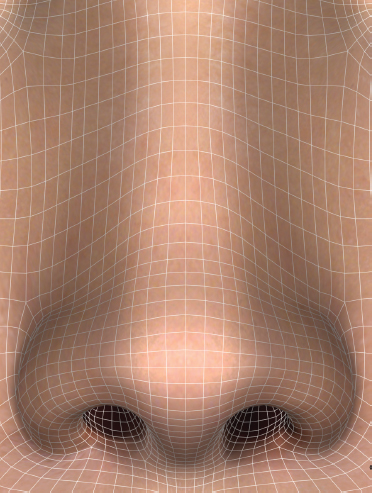
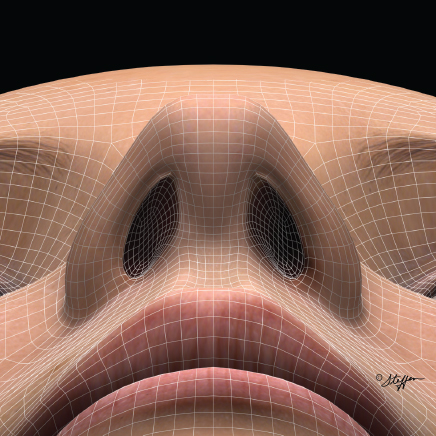
Important information about the columella, alar base, lobule, and nostrils is obtained on base view. The nose should have a rounded, equilateral triangular shape without any pinching or concavities between the tip and alar lobules on base view ( Fig. 33.8 ). 11 External nasal valve collapse is also best assessed on this view, which manifests as inward collapse of the nostril margin (alar collapse) upon inspiration. Various grafting techniques exist to surgically correct external valve collapse and are covered elsewhere in this book. 9 , 12
On lateral view (or profile view), which tends to be more forgiving than the frontal view, the dorsum is assessed for radix/nasal starting point position, smoothness, contour, and the presence of a supratip break. Tip projection and rotation, nasal length, the nasolabial angle, and the double-break (or columellar-lobular angle) are also analyzed. The position and inclination of the nasofrontal and nasolabial angles must be carefully evaluated. The deepest point of the nasofrontal angle or radix, the sellion, corresponds to the nasal starting point and should lie at or just below the superior palpebral fold in women, and at or just above the superior palpebral fold in men. 3 A blunted nasofrontal angle (which should approximate 120 degrees, although it may vary based on forehead shape) may be due to a bony prominence in this region or a thick procerus muscle. Both may be corrected through judicious excision of bone or muscle to create a welldefined nasal starting point. Conversely, a low or deep radix may require placement of a subperiosteal radix graft, which leads to an apparent lengthening of the nose. An overly acute or blunted nasolabial angle (which should normally range from 90 to 95 degrees in men and 95 to 110 degrees in women) may be partially effaced through (1) placement of a footplate suture if flaring medial crural footplates are present, (2) through placement of cartilage plumping grafts at the columella–labial junction, or (3) through placement of larger premaxillary plumping grafts via a sublabial incision in more severe cases as may be seen in non-Caucasian noses ( Fig. 33.9 ). 13
Intranasal Exam
The intranasal exam should be performed via anterior rhinoscopy and rigid endoscopy (0- or 30-degree telescopes). It should examine the inferior turbinates, nasal septum, and patency of the internal nasal valves. A narrow internal nasal valve, septal deviation, inferior turbinate hypertrophy, or mucosal synechiae may lead to nasal obstruction and must be corrected during surgery.
In the vast majority of patients, resection of the inferior turbinates, which can lead to nasal dryness and atrophic rhinitis if performed too aggressively, is not necessary after an adequate septoplasty is performed. However, if inferior turbinate reduction is necessary due to compensatory enlargement, it should be done conservatively in a submucosal technique to leave the medial mucosa intact.
The nasal septum needs to be evaluated for deviation and perforation. Not only does it contribute to nasal airway resistance if deviated, but it also is the most important donor site for grafting purposes. Identification of a deviated ethmoid plate is also important as it may be the culprit for nasal obstruction after osteotomies and infracture of the bony sidewalls.
To assess for patency of the internal nasal valves, a Cottle or modified Cottle maneuver is performed with lateral cheek tension or the use of an instrument to lateralize the sidewall of the nose, respectively. If dynamic collapse occurs upon inspiration, internal nasal valve patency may be improved through either strengthening the sidewalls with alar batten and/or lateral crural strut grafts (LCSGs), or managing the middle nasal vault with placement of spreader grafts.
Photography and Imaging
Photography
Standard and uniform color photographs before and after surgery are important to document a patient’s deformity and how it has been corrected surgically. Beyond medicolegal utility, photography is an important tool in operative planning and execution. The traditional 35-mm color slides have been replaced by digital photography in the standard six head positions (full frontal, right and left lateral, right and left oblique, and basal views). Use of a standard 105-mm portrait lens with two light sources positioned above and 45 degrees from the patient (seated in front of a light blue background) is ideal. Additional useful photo documentation includes fullface frontal, right and left lateral, and close-up frontal smile views. Attention should be paid to the close-up frontal smile view. Patients with smile patterns where the oral commissures are the highest point of the lips upon smiling are at risk for upper lip creasing when suturing a caudal septal extension graft or columellar strut to the anterior nasal spine. Those patients should be treated with grafts that are just short of and not sutured to the nasal spine ( Fig. 33.10 ).

Imaging
Computer imaging is useful in facilitating communication between the surgeon and the patient. Oftentimes, patients have difficulty expressing their desires and surgical goals in words. Imaging also aff ords the surgeon the possibility to illustrate realistic and surgically attainable changes to the patient. However, it is very important to perform computer imaging conservatively to not create unrealistic expectations and hopes in the patient.
Imaging on frontal view is more difficult than on profile view because the nose is contrasted against the flesh-colored background of the face. However, shadows may still be moved in sophisticated computer programs on frontal view to illustrate possible changes. The profile view is easier to manipulate in twodimensional imaging programs as the skin is contrasted against a blue background. Profile alignment, tip projection and rotation, the alarcolumellar relationship, nasal length, and chin projection are amongst the most common parameters addressed on computer imaging. Finally, it must be emphasized to the patient that computer images serve as proposed changes only rather than guaranteeing a final result. Newer threedimensional imaging software that requires special cameras is increasing in popularity but is beyond the scope of this chapter.
Grafting
Rhinoplasty requires grafting material, which is typically abundantly present in primary cases but frequently insufficient in secondary surgery. Therefore, secondary donor sites are often necessary in revision operations as anatomical structures may require reconstruction with grafting materials that can be carved and shaped. Grafting material may be classified based on its donor site, functional role, or origin.
Structural vs. Contour Grafts
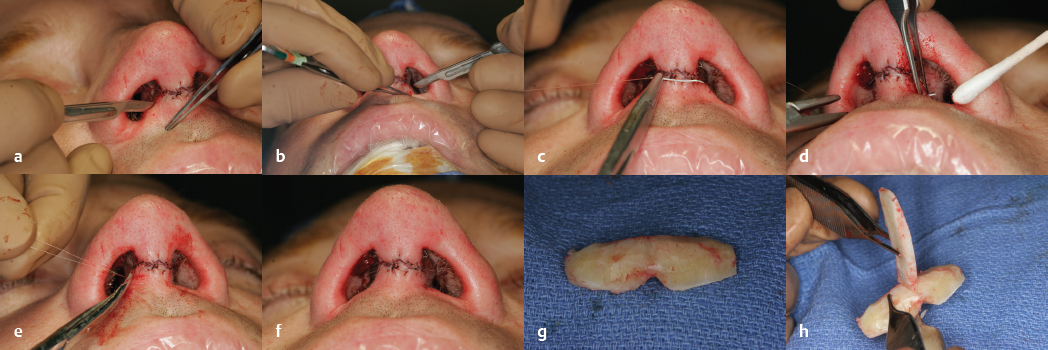
Cartilage grafts may be classified as structural or contour grafts, depending on their role. Structural grafts, as the name implies, serve a supportive function to support the skeletal framework. In general terms, favorable donor sites for structural grafts are septal cartilage, ear cartilage, and rib cartilage. With that in mind, surgeon skill, preference, and experience, in combination with structural demands of the patient, play an integral role in determining which donor site is most appropriate for a given graft. For instance, caudal septal extension grafts tolerate postoperative warping the least and, if possible, rib grafts should be either avoided or splinted. Spreader grafts, on the other hand, may tolerate a slight curvature, and costal cartilage might be rather favorable for that purpose particularly in the presence of a deviated dorsum. In such cases, the slight curvature of a carved costal cartilage graft may be used to one’s advantage to help straighten the deviated nose. Alternatively, the two concave surfaces of the opposing spreader grafts may face each other to counteract their tendency to warp ( Fig. 33.11 ).
Since contour grafts serve less of a functional but rather an aesthetic role, graft stability and rigidity are less critical factors. As a matter of fact, contour grafts with softer consistencies are preferred, as placement is closer to the skin with the possibility of undesirable postoperative palpability. Favorable donor sites for contour grafts are morselized septal cartilage, auricular, or lower lateral cartilages.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


