31 Facial Analysis of the Rhinoplasty Patient
Introduction
The standards of facial beauty vary in different cultures and are known to change over time, eluding objective definition. Facial beauty may be characterized by a combination of factors that involve symmetry and aesthetically pleasing proportions and relationships. For centuries Greek artists highlighted their personal sense of facial proportion in their drawings often using them to reflect their subject’s temperament. Modern day anthropometric measurements of fixed skeletal and soft tissue points have allowed a more objective and quantitative analysis of the face in the form of ratios, lengths, and angles. In the last decade mathematicians and computer scientists have attempted to define facial beauty using fractal geometry and digital analysis. 1 , 2 One conclusion has been that facial beauty correlates with simplicity relative to the subjective observer’s way of encoding and memorizing it. In other words, “beauty is in the eye of the beholder” and any attempts to quantify facial beauty have to take the observer into account. Even so, facial beauty appears to universally esteem certain geometric rules of proportions, angles, symmetry, and balance. A comprehensive understanding of these proportions, angles, measurements, and relationships that are considered to be the standard for the attractive face is requisite to identifying deviations from the ideal. Although the aesthetic analytical ideals for Caucasian patients are well categorized, ethnic variations from these standards have not been well characterized. Thus attempts to transpose uniform standards on diverse ethnic facial platforms have often resulted in gross disharmony and dissatisfied patients. Successful rhinoplasty absolutely depends on accurate and thorough analysis of both the nose and the surrounding facial features with an in-depth appreciation for set analytical standards, ethnic variations, and the patient’s desires. The purpose of this chapter is to present clinically applicable aesthetic concepts of the nose and the face that are helpful in evaluating a patient for rhinoplasty. It focuses on the analytic details for the Caucasian patient but highlights the anatomical variants in non-Caucasian patients.
An essential concept that must be emphasized is that regardless of the ethnic patient base or the analytic details that a surgeon chooses, it is important to have a comprehensive and consistent system to evaluate the nose to avoid distraction by a single feature. Moreover, a thorough analysis will predict the underlying structural anatomy and anticipate surgical technique or maneuvers that will be employed to create the desired changes. A comprehensive approach, which is shared with the patient, helps to clarify aesthetic and physiologic goals of the surgery. In essence, a thorough analysis will help the surgeon to rehearse the surgery. In the end, facial harmony is an essential goal of surgery and some rhinoplasty surgeons feel that an attractive nose draws attention to the eyes, which are the focus of social interaction. A meaningful component of facial harmony includes contours that have gentle curves with areas of highlight and shadow. Unnatural contours such as a bossa and sharp lines distract from other attractive facial features.
Nasal–Facial Analysis
Analysis of the patient prior to rhinoplasty begins with the assessment of nasal–facial relationships. Although there is great variety in nasal and facial appearances, general guidelines regarding attractive nasal–facial proportions have been developed. 3 There have also been many different methods for analyzing facial proportions, some of which involve intricate and confusing measurements that are difficult to apply. The following diagrams provide some basic guidelines that are easy to apply both pre- and intraoperatively for the rhinoplasty patient.
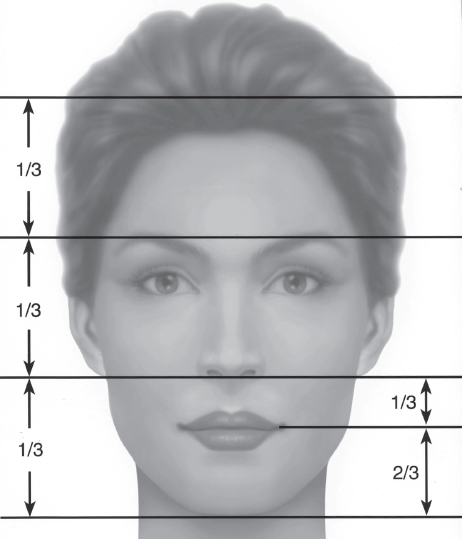
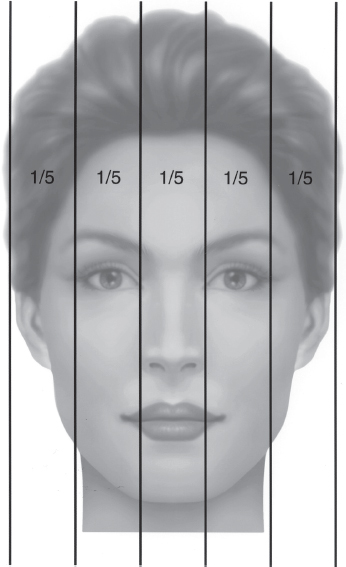
The face has classically been divided by horizontal lines into thirds ( Fig. 31.1 ). The forehead hairline (trichion) to the glabella, the glabella to the nasal base (subnasale), and the nasal base to the chin (menton) are approximately equal thirds. Powell and Humphrey noted that because of the variable position of the hairline, the “upper third” portion was not significant except in procedures such as forehead lifts. 3 Accordingly, they redefined the evaluation of facial heights with the middle third originating from the nasion and extending to the subnasale. With these redefined boundaries, the middle third approximated 43% and the lower third 57%, respectively, of the distance from the nasion to the menton. The lower third of the face may be further subdivided into thirds, with the upper lip being one-third and the lower lip and chin twothirds. The nose and face may be divided by vertical lines into horizontal facial fifths, with the nasal base width equal to the intercanthal distance and the width of each eye ( Fig. 31.2 ).
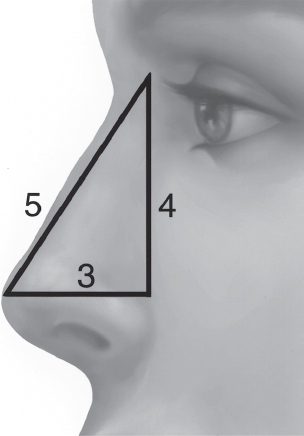
When viewed in profile, the nose should project from the face with the proportions of a right-angle triangle with the nasal projection being 60% of the nasal length ( Fig. 31.3 ). 4 The nasofrontal angle begins approximately at the level of the supratarsal crease, and the chin should approximate the lower lip in its anterior projection.
Within these general aesthetic guidelines, variations exist due to individual or ethnic differences. African American, East Asian, and Latino noses often deviate from the classic description of vertical fifths and horizontal thirds. The nasal base width among these ethnic groups is often wider than the intercanthal distance and may be better related to the intracaruncle distance. The middle third from the nasion to the subnasale in the Middle Eastern patient is frequently longer than the lower third but is shorter in East Asian and African American patients.
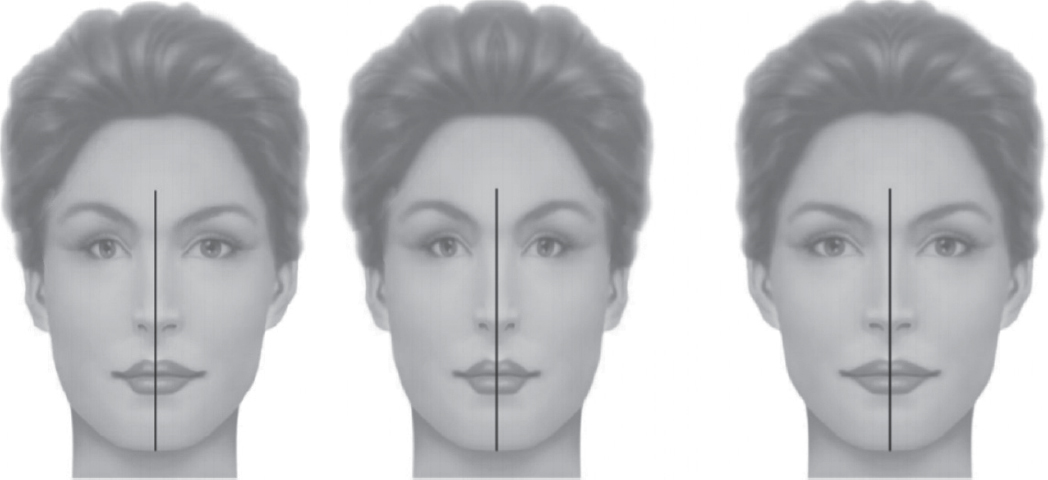
Most patients have facial and nasal asymmetries that should be discussed in the preoperative consultation. This is best demonstrated by using computer formatting of digital photographs to create two faces from different facial halves ( Fig. 31.4 ). These asymmetries may not be noticed by the patient preoperatively; however, there is an increased likelihood that the patient will be hypervigilant to irregularities after surgery. Moreover, skeletal asymmetry, as in the case of a crooked nose resting on a deviated nasal spine and philtral column, may compromise the final result if not recognized and appropriately addressed.
Nasal Evaluation
As noted earlier in the discussion, a systematic approach is essential. It includes excellent facial photography that not only documents the preoperative appearance of the nose, but it is an essential resource for study prior to surgery and a resource for introspection postoperatively. A focused nasal evaluation includes evaluating the character of the skin envelope followed by a frontal analysis and profile evaluation. Considerable insight can be derived from analysis of the base view. Additional details from oblique and supplementary views such as the sky or helicopter view, and the appearance with smiling yield additional value information. Finally, we employ a checklist of several analytic features that are associated with adverse outcome and require surgical accommodation. This list is presented toward the end of the chapter.
Nasal Skin
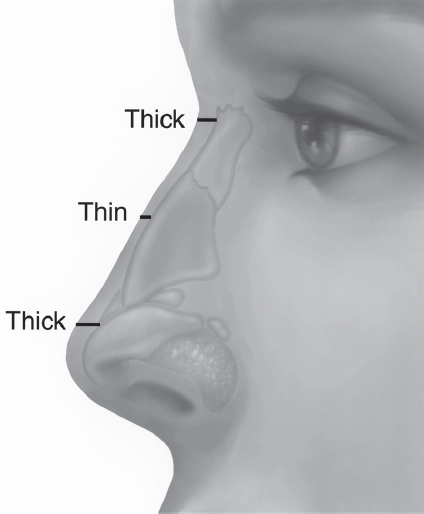
The evaluation of the rhinoplasty patient should take into account the skin and soft tissue covering of the nose. Nasal skin that is thick and sebaceous does not drape well to reveal subtle changes that have been made in the bony cartilaginous framework. Thus reduction rhinoplasty in patients with thick skin may produce a smaller but poorly defined nose, whereas less aggressive reduction combined with judicious placement of cartilage grafts will result in a more balanced and refined appearance with preservation of airway. Many surgeons feel that edema takes longer to subside before the final results are apparent when thick, sebaceous skin is present. However, thin skin may drape too well, showing any minor deformities and irregularities underneath.
Nasal skin is generally thicker at the nasofrontal angle and becomes thinner over the rhinion ( Fig. 31.5 ). From the rhinion to the supratip the skin becomes thicker again, with an increase in sebaceous glands. Over the nasal tip the skin may vary considerably from thin skin that outlines the underlying nasal tip cartilages to thicker skin that contributes to the bulbosity of the tip. The alar lobule skin is also thick, with a greater density of sebaceous glands, whereas the skin of the columella is generally thinner than any area of the nose.
The presence of previous scars (chicken pox, traumatic, etc.) should be noted as they may affect how the soft tissue redrapes and may require camouflaging techniques. Signs of acne rosacea should prompt pretreatment or referral to a dermatologist because it may become exacerbated postoperatively with persistent erythema.
Framework Strength
Palpation of the bony and cartilaginous framework is an essential part of rhinoplasty analysis. For example, the stiffness of the lower lateral cartilages will influence rhinoplasty technique. Weak cartilage may require more conservative trimming or augmentation to achieve the desired contour and offset the contractive forces of healing. Conversely, stiff cartilage may require more aggressive modification. Short nasal bones likewise will alter the surgical approach. When short nasal bones are present there is a corresponding increased length in the cartilaginous vault. The pliable nature of the cartilage makes the middle third of the nose more vulnerable to distortion generated by the contractive forces of healing. This is particularly true when a dorsal hump is reduced and the new dorsal edge of the septum is thinner than the original. Rhinoplasty in the presence of short nasal bones and a very pliable cartilaginous frame will often require reenforcing structural grafts, such as spreader grafts or flaps. Preservation of the structural support of the airway is mandatory. Aesthetic enhancement at the cost of physiological compromise will not benefit the patient.
Frontal View
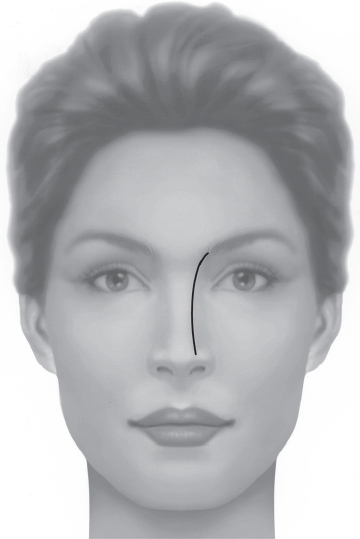
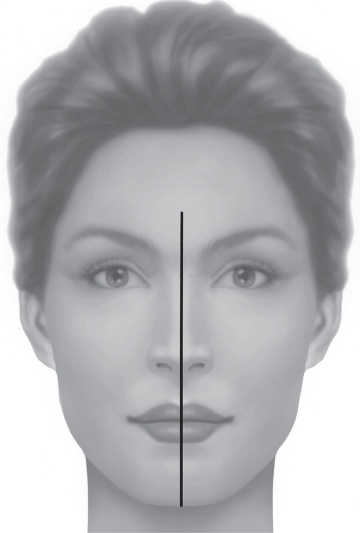
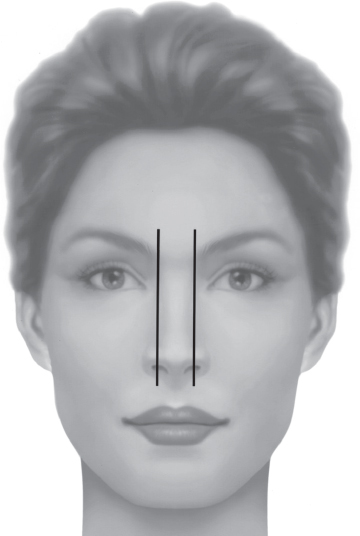
On frontal view the symmetry of the nose can be evaluated. A curved unbroken line can be viewed sweeping from the medial brow to the ipsilateral nasal tip defining point ( Fig. 31.6 ). 5 A line from the midglabella to the menton should bisect the nasal bridge and tip ( Fig. 31.7 ). Any deviation or twist of the external nose should be readily apparent from this view. The width of the nasal dorsum and alar base can best be assessed from a frontal view. The width of the alar base should be approximately the same width as the intercanthal distance, but must include ethnic variations, as mentioned previously. If the alar base is significantly wider than the intercanthal distance, alar base modification can be considered and is discussed further in the section on the base view ( Fig. 31.8 ).
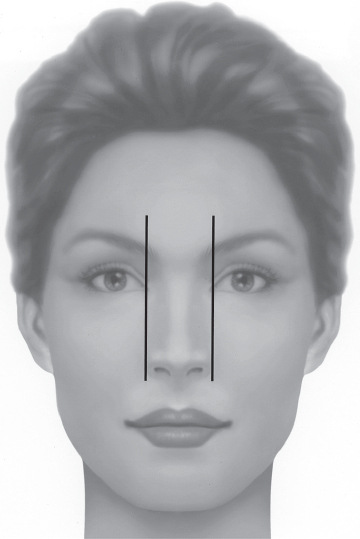
The width of the bony sidewall of the nose should be 75 to 80% of the normal alar base ( Fig. 31.9 ). If the bony base exceeds this dimension, narrowing can be accomplished at the time of lateral osteotomy. If the width of the bony base is within the normal range but the bony dorsum is wide, mobilization of the nasal bones will be required while keeping the bony base width the same.
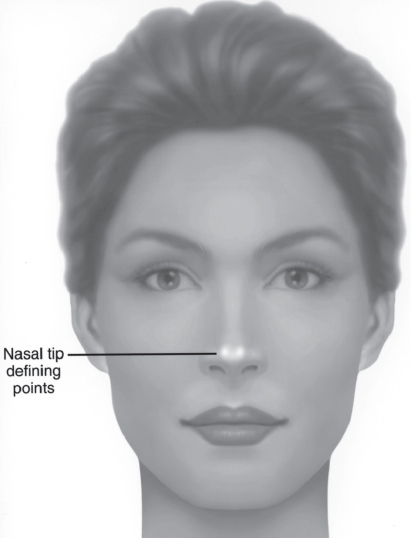
On frontal view the nasal tip has two tip defining points that represent light reflection on the skin overlying the domes of the lower lateral cartilages. This distance is normally 6 to 8 mm in the attractive Caucasian nose ( Fig. 31.10 ). Another helpful guideline for the tip defining points is that the distance from the tip defining points to a horizontal line across the lower edge of the alar margin should approximate the distance from the line to the caudal edge of the columella ( Fig. 31.11a ). Asymmetries in the domes of the lower lateral cartilage will be seen as tip asymmetries on frontal view that may require tip modification during surgery. Bulbosity of the nasal tip should be noted and potential causes delineated. A bulbous, illdefined tip may result from several variations including overly widened lateral alar crura, very thick sebaceous skin draping over normal cartilages, divergent interdomal angle, wide intradomal arch, and lateral crural cephalic malposition. The technique employed to achieve tip definition relies on accurate analysis of these contour-defining characteristics of the nasal tip and alar lobule. If an excessive distance is found between the tip defining points, the domes of the lower lateral cartilage may be brought closer together at surgery by a variety of techniques, including interdomal and intradomal suturing. It is particularly important to identify the malpositioned lateral crus because ill-conceived attempts at tip definition with cephalic trimming without appropriate compensatory measures may result in delayed pinching and valve collapse. The normal angulation of the lateral crus is 15 degrees, whereas in cephalic malpositioning the slant could be up to 60 degrees, bestowing the nasal tip the “parenthesis” appearance.
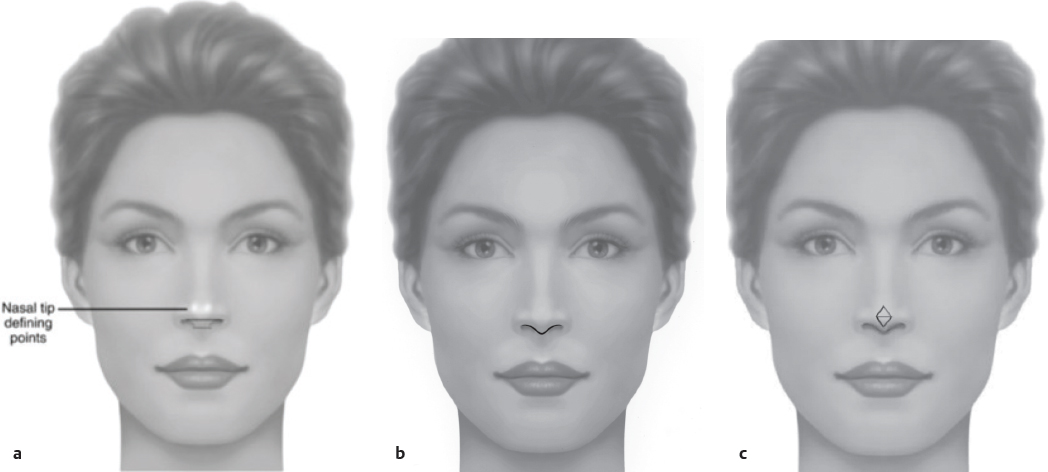
The columella is seen to hang just inferior to the alar rims, giving the infratip lobule a gentle “gull in flight” appearance on frontal view ( Fig. 31.11b ). 6 Excessive dependence of the columella on frontal view most often indicates a protruding or hanging columella, which may require reduction. Lack of this columella contour on frontal view signifies a retracted columella, which will need augmentation. Nostril show should not be excessive indicating the nasal tip is overly rotated. Any asymmetries of the alar rim or its attachment at the alar base should be noted at this time. Lateral hooding of the alar rim is best seen on the frontal view and may be addressed with specific techniques to provide tip harmony.
On frontal view, the refined tip reflects the double-break appearance of the supratip and infratip. The supratip is defined by the junction of the nasal dorsum and the nasal tip, and the infratip by the junction of the tip and columella. The relationship between the infratip break, the tipdefining points, and the supratip dip can be delineated by two imaginary equilateral triangles ( Fig. 31.11c ).
A discussion of guidelines regarding proper dimensions on frontal view must be tempered by evaluation of the nose from other projections as well as consideration of harmony with other facial proportions and ethnic variations. For example, if the middle third of the face is long and the intercanthal distance is narrow, narrowing the alar base to match the intercanthal distance may cause the nose to appear excessively long and draw additional attention to the long midface. Likewise, attempts to narrow the nasal base in some ethnic noses to match the intercanthal distance may result in an unnatural appearance and functionally compromised stenotic nostrils. Recognition of these nuances and the ability to modify surgical technique to accommodate them differentiates the superior rhinoplasty surgeon from the average.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


