26 Orbital Wall Blowout Fractures
Abstract
“Orbital Wall Blowout Fractures” discusses fractures of the thin bone of the orbital floor, the medial orbital wall, or both. Such a fracture is called “pure” when the bony orbital margin is intact and “impure” when the orbital wall fracture is accompanied by a fracture of the orbital rim, for example as part of a zygomatic complex fracture. Pure orbital wall blowout fractures can be due to backward displacement of the eyeball caused by a blunt non-penetrating object, raising the intraorbital pressure sufficiently to fracture the thin medial orbital wall or the bone of the orbital floor, or to a transient deformation of the orbital rim transmitting the force of injury directly to the orbital wall. These fractures may occur after any blunt trauma to the periorbital region, for example after a blow with a fist. The breakage of the weak areas of the orbital wall provides pressure relief, allowing the orbital tissues to move into the maxillary antrum or ethmoid air cells rather than being crushed. If the eyeball ruptures, the patient also has an orbital wall blowout fracture until proven otherwise.
26.1 Introduction
The term pure orbital blowout fracture is used to describe a fracture of the orbital floor, the medial orbital wall, or both, with an intact bony orbital margin. The term impure orbital blowout fracture is used when such fractures occur in conjunction with a fracture of the orbital rim, for example as part of a zygomatic complex fracture. The most common site for a blowout fracture to occur is the posteromedial aspect of the orbital floor medial to the infraorbital neurovascular bundle where the maxillary bone is very thin. Because the lamina papyracea is also very thin, the medial orbital wall is also prone to fracture, either in isolation or in association with a fracture of the orbital floor or other facial bones.
26.2 Etiology
Two mechanisms are believed to be responsible for pure orbital wall blowout fractures:
The backward displacement of the globe caused by a blunt nonpenetrating object, such as a tennis ball, which raises the intraorbital pressure sufficiently to fracture the posteromedial orbital floor and/or the lamina papyracea of the ethmoid.
A transient deformation of the orbital rim transmits the force of injury directly to the orbital wall.
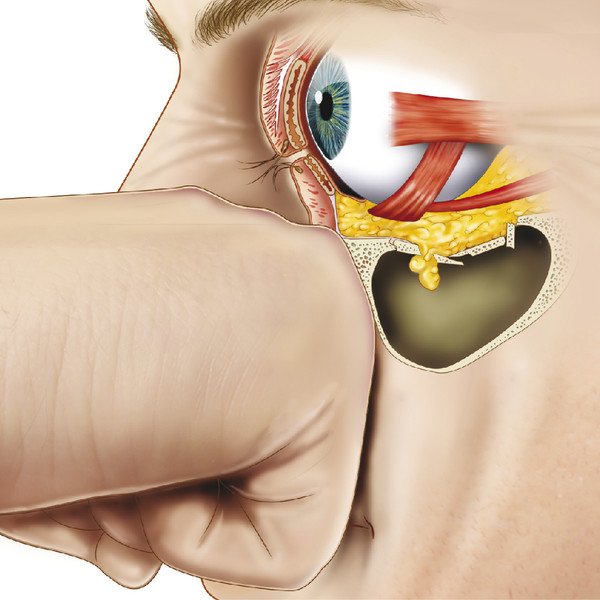
These fractures may occur after any blunt trauma to the periorbital region, for example after a blow with a fist (Fig. 26‑1). The weak areas of the orbital walls provide some means of protection to the globe and orbital tissues, permitting them to expand into the maxillary antrum and/or ethmoid sinus rather than being compressed against the other more rigid areas of the orbit. The periorbita overlying the fracture is usually ruptured, allowing the adjacent orbital fat to prolapse into the fracture site. Occasionally part of an adjacent extraocular muscle will also prolapse into the fracture site.
Although a rupture of the globe can complicate such fractures, this occurrence is rare. Conversely, any patient who has suffered blunt trauma sufficiently severe to cause a ruptured globe has an orbital wall blowout fracture until proven otherwise.
26.3 Diagnosis
A high index of suspicion should be maintained for the presence of a blowout fracture in any patient who has sustained blunt periorbital trauma. The patient’s clinical signs will depend on the timing of the examination in relation to the traumatic episode. A patient presenting several months after the traumatic event may have enophthalmos as the only physical sign.
26.3.1 Clinical Signs and Symptoms
The following clinical signs and symptoms may be associated with an orbital wall blowout fracture:
Eyelid ecchymosis or hematoma.
Subcutaneous emphysema.
A neurosensory loss in the distribution of the infraorbital nerve.
A limitation of ocular motility with diplopia.
Enophthalmos, proptosis, or hypoglobus.
An upper eyelid sulcus deformity.
Pseudoptosis.
Headache.
Nausea or vomiting.
Bradycardia.
Eyelid Ecchymosis or Hematoma
Although eyelid ecchymosis, hematoma, or edema are usually present when the patient is seen soon after trauma has occurred, these signs may be absent, as seen in the so-called white-eyed blowout fracture in pediatric patients. In these patients, the flexible bone of the orbital floor is fractured and forced inferiorly. The periorbita is ruptured, resulting in a prolapse of inferior orbital fat. Part of the inferior rectus muscle may also be forced into the fracture. The flexible bone of the orbital floor then springs back into position, causing a severe entrapment of the prolapsed tissues.
Subcutaneous Emphysema
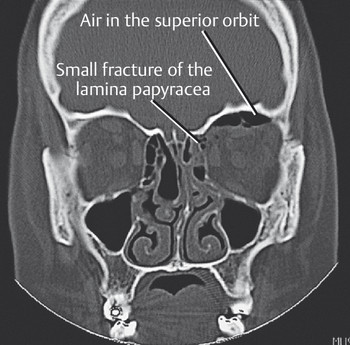
A blowout fracture communicates with an air-filled sinus. Air may be forced into the orbit and/or eyelids, particularly in medial orbital wall blowout fractures, when the patient blows the nose or sneezes. Subcutaneous emphysema may result in palpable crepitus. Patients should be urged not to blow their nose or to hold the nose when sneezing, or the subcutaneous emphysema may be greatly exacerbated. Very rarely, air forced into the orbit can cause a severe proptosis and an orbital compartment syndrome with a compromise of the blood supply to the optic nerve or globe (Fig. 26‑2).
Neurosensory Loss in the Distribution of the Infraorbital Nerve
Dysfunction of the infraorbital nerve is almost pathognomonic of an orbital floor blowout fracture. The patient is usually aware of altered sensation in the ipsilateral cheek, upper teeth, and upper lip. This occurs because the fracture extends along the infraorbital groove or canal, injuring the infraorbital nerve. Not all patients with an orbital floor blowout fracture, however, experience such sensory deficits. These annoying sensory deficits tend to resolve spontaneously with time but may be exacerbated by surgical intervention for the fracture. Very rarely, persistent pain in the distribution of the infraorbital nerve may be an indication for surgical decompression of the nerve, which may be compressed by bone fragments.
Limitation of Ocular Motility
A patient with an orbital floor blowout fracture may have vertical diplopia related to a variety of different mechanisms. Horizontal diplopia in the presence of a medial orbital wall blowout fracture is less common. The following mechanisms may be responsible for limitation of ocular motility:
Entrapment of connective tissue septa or of an extraocular muscle within the fracture.
Hematoma and/or edema in the orbital fat adjacent to the fracture.
Hematoma or contusion of an extraocular muscle.
Palsy of an extraocular muscle related to neuronal damage.
Volkmann’s ischemic contracture of an entrapped extraocular muscle.
Enophthalmos, Proptosis, or Hypoglobus
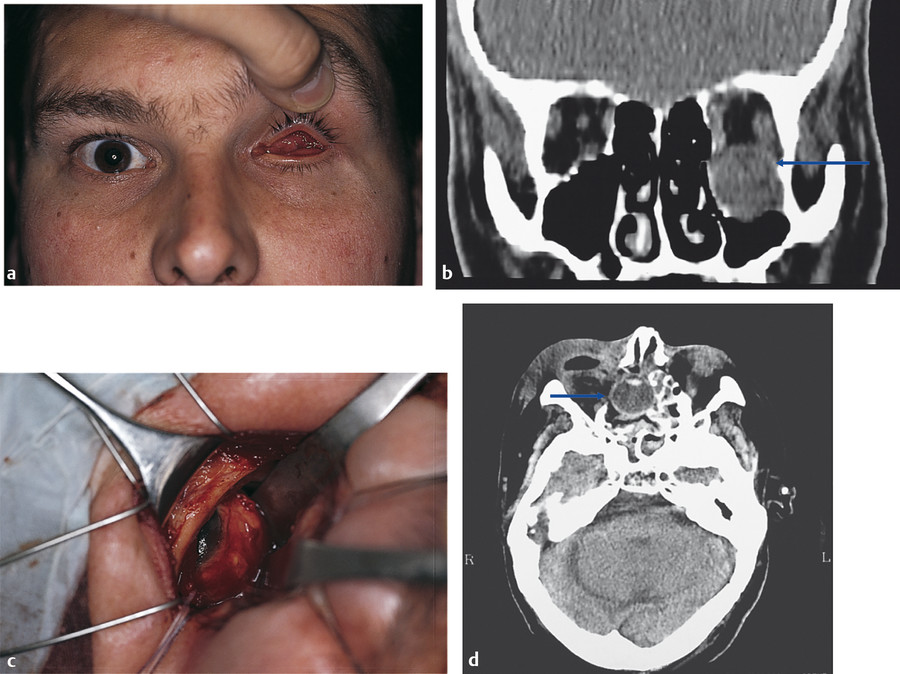
Enophthalmos is produced by an enlarged orbital volume and varies from insignificant to cosmetically disfiguring depending on the degree of orbital bony expansion. Fat atrophy usually contributes little if anything to the enophthalmos. Enophthalmos may be masked by orbital hematoma, edema, or air, which may even cause proptosis in the first few days after trauma. Proptosis, however, may be associated with a “blowin” fracture if the fragmented bones of the orbital floor are displaced into the orbit. This is more common in the context of fractures involving the roof of the orbit. Enophthalmos is always significant in the presence of combined fractures of the orbital floor and medial orbital wall. Hypoglobus is seen in the presence of extensive orbital floor blowout fractures. In some patients, the maxillary antrum extends laterally for some distance beyond the infraorbital neurovascular bundle, with the ensuing orbital floor defect occupying almost the whole orbital floor. Very rarely, the globe may come to lie within the maxillary antrum or even within the ethmoid sinus (Fig. 26‑3).
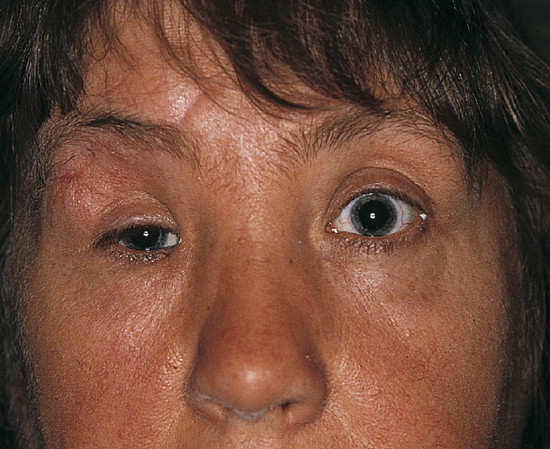
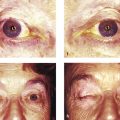
Upper Eyelid Sulcus Deformity or Pseudoptosis
Enophthalmos results in a decreased support of the upper eyelid, which in turn leads to a secondary pseudoptosis and an upper eyelid sulcus deformity (Fig. 26‑4).
Headache, Nausea, Vomiting, and Bradycardia
In pediatric patients with a white-eyed blowout fracture, the symptoms of headache with nausea and vomiting associated with a bradycardia may be misinterpreted as signs of blunt head trauma requiring admission to the hospital for head injury observations. These symptoms and signs in the presence of such a fracture are produced by the oculocardiac reflex.
26.3.2 Clinical Evaluation
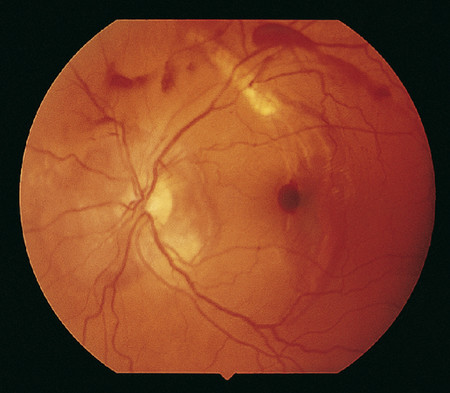
Any patient who has sustained blunt orbital trauma should undergo a complete ophthalmic examination to exclude associated ocular injuries (Box 26.1; Fig. 26‑5). The incidence of ocular injuries has been reported as 14 to 30%. The possibility of a globe rupture must always be considered and excluded before a forced-duction test is performed.
Box 26.1 Ocular Injuries Complicating Blowout Fractures
Globe rupture
Retinal tears
Retinal dialysis
Vitreous hemorrhage
Angle recession
Hyphema
Lens subluxation
Traumatic cataract
Choroidal rupture
Commotio retinae
Macular scarring
Traumatic mydriasis
Any proptosis or enophthalmos should be measured using a Hertel exophthalmometer. Any vertical displacement of the globe should also be measured and recorded. The eyelids and periorbital tissues should be palpated for subcutaneous emphysema and for any orbital rim fractures. The malar eminences should be palpated and any depression or displacement noted (Fig. 26‑6).

The patient should be asked to open and close his or her mouth to ensure there is no associated pain or trismus. Such signs and symptoms are suggestive of a zygomatic complex fracture. A record of the extent of any infraorbital sensory loss should be made.
A full orthoptic assessment should be performed with prism measurements in nine positions of gaze, a Hess chart, and a monocular and binocular visual field assessment. A forced-duction test and an active force-generation test should be performed. Before the performance of a forced-duction test, a cotton-tipped applicator is soaked with topical anesthetic drops and held against the limbus for a few minutes. The patient should be recumbent. Fine-toothed forceps are then used to grasp the conjunctiva and Tenon’s capsule just posterior to the limbus. The patient is then asked to look in the direction of restriction of movement of the eye while the examiner attempts to move the globe in the same direction (Fig. 26‑7). A patient with tissue entrapment will usually experience pain on attempted globe movement in the direction of restriction. The results of this test need to be interpreted with caution. If the examiner is unable to move the globe normally, this implies entrapment of the inferior orbital septa, but a positive forced-duction test can also be caused by extraocular muscle or orbital hematoma and edema. A strongly positive forced-duction test in a patient with evidence of a blowout fracture on computed tomography (CT) does suggest tissue entrapment as the cause of ocular restriction.

In an active force-generation test, the globe is again grasped with fine-toothed forceps and the patient asked to try as hard as possible to move the eye in the direction of action of the muscle under investigation. The examiner can feel muscle contraction from a tug on the forceps. An active force-generation test is useful in differentiating extraocular muscle paralysis from tissue entrapment.
If a patient has symptoms and signs suggestive of an orbital wall blowout fracture, CT should be performed in an axial plane with coronal and sagittal reconstructions (Fig. 26‑8). With modern CT scanners, this investigation can be performed very quickly. Images available in three planes are extremely valuable in assessing the full extent of the injury. A plain skull radiograph is of little use in the evaluation of a blowout fracture. CT demonstrates the relationship of the soft tissues to the fracture sites, permits an evaluation of any secondary effects of trauma (e.g., retrobulbar hemorrhage, intraoptic nerve sheath hematoma, or subperiosteal hematoma), and can help to demonstrate any complications of trauma (e.g., orbital cellulitis, orbital or subperiosteal abscess, and retained orbital foreign bodies).

Key Point
In a pediatric patient with a white-eyed blowout fracture, there may be very little evidence of a fracture on CT, and the scan may be reported by a radiologist as showing no fracture.
26.3.3 Management
Patients should be urged not to blow their nose or to hold their nose when sneezing. The role of antibiotic prophylaxis is controversial. If CT shows evidence of chronic sinusitis, antibiotics should be prescribed to prevent a secondary orbital cellulitis (Fig. 26‑9).

A number of different surgical specialties may be involved in the management of patients with an orbital wall blowout fracture, and opinions differ concerning the indications for surgery, the timing of surgery, the surgical approach, and the use of orbital implant materials. In general, the following are indications for the surgical repair of a blowout fracture:
Soft tissue entrapment with disabling diplopia that is failing to resolve.
Enophthalmos greater than 2 mm.
CT evidence of a large fracture.
The indications are, however, relative and not absolute. The decision to operate should be considered very carefully for the individual patient, taking into account the patient’s wishes and the risks and potential complications of surgery.
Patients with diplopia are observed for a period of approximately 2 to 3 weeks. If the diplopia resolves with a small fracture evident on CT, no surgical intervention is required.
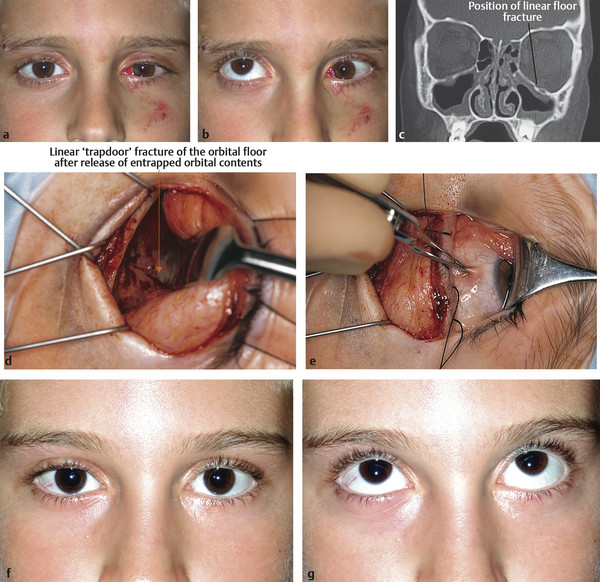
There is an important exception to this. Pediatric patients with marked tissue entrapment and a linear fracture on CT (a “trapdoor” fracture) are at risk of developing an ischemic contracture unless the tissue entrapment is released very early (Fig. 26‑10; Video 26.1). This is an indication for urgent surgery.
Key Point
An orbital wall blowout fracture in a pediatric patient should be evaluated urgently and in the presence of restriction of ocular motility may require surgical intervention without delay.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


