3 Lower Eyelid Entropion
Abstract
“Lower Eyelid Entropion” discusses an eyelid malposition in which the lower eyelid margin is turned inward against the eyeball. The keratinized skin of the eyelid margin and the eyelashes rub against the inferior cornea and bulbar conjunctiva, causing irritation, inflammation, and discharge. Patients with a lower lid entropion tend to seek medical attention early because of the troublesome symptoms. The condition can be due to failure of the lower eyelid retractor muscles (most often in old age), scarring, or spasm, or it may be congenital. This chapter describes all surgical procedures and postoperative care in each instance in detail.
3.1 Introduction
Lower eyelid entropion is an eyelid malposition in which the lower eyelid margin is turned inward against the globe. The keratinized skin of the eyelid margin and the eyelashes rub against the inferior cornea and bulbar conjunctiva, causing irritation, inflammation, and discharge. Patients with a lower lid entropion tend to seek medical attention early because of the troublesome symptoms. Lower lid entropion can be classified into four types.
3.2 Classification
3.2.1 Involutional Entropion
Most entropions are involutional and therefore seen in older patients. In the lower eyelid, involutional changes typically result in either a lower lid entropion or ectropion, whereas in the upper eyelid the same changes result in ptosis. A combination of factors has been proposed to account for the eyelid malposition (Fig. 3‑1):
Laxity, dehiscence, or disinsertion of the lower eyelid retractors ( Fig. 3‑1a).
Overriding of the preseptal orbicularis oculi muscle over the pretarsal orbicularis oculi muscle.
Horizontal eyelid laxity.
Enophthalmos.
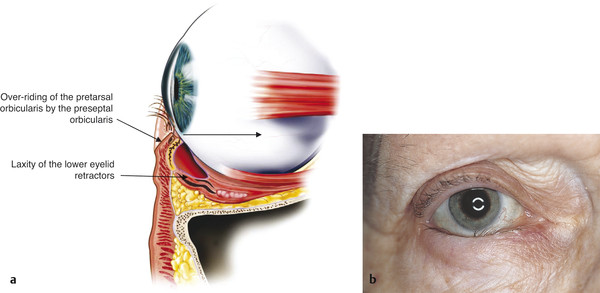
Any surgical treatment should aim to address these factors, with the exception of enophthalmos. Enophthalmos has not been shown to be a significant factor in the etiology of involutional lower eyelid entropion. Laxity, dehiscence, or disinsertion of the lower eyelid retractors is the primary cause of involutional entropion. This lower eyelid retractor problem allows the inferior edge of the tarsus to rotate away from the globe. Horizontal eyelid laxity leads to instability of the eyelid. The preseptal orbicularis appears to force the lower eyelid margin inward.
Key Point
Laxity of the eyelid retractors is the primary cause of involutional lower eyelid entropion.
3.2.2 Cicatricial Entropion
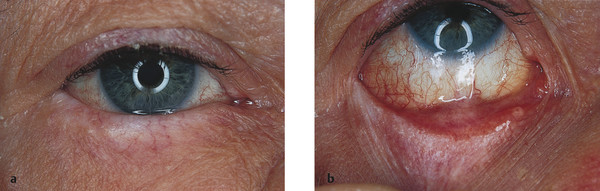
Any condition that causes contracture of the conjunctiva can result in a cicatricial entropion (Fig. 3‑2). Such conditions include chemical burns, surgical or accidental trauma, topical glaucoma medications, ocular cicatricial pemphigoid, trachoma, and Stevens-Johnson syndrome. It may also occur with the extrusion of an orbital floor implant through the inferior fornix.
3.2.3 Acute Spastic Entropion
Acute spastic entropion is seen in susceptible individuals with blepharospasm that has been induced by ocular irritation. Although treatment of the underlying cause of ocular irritation may reverse the eyelid malposition, a permanent entropion may ensue that will require surgical intervention.
3.2.4 Congenital Entropion
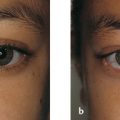
Congenital lower eyelid entropion is a rare condition. It differs from congenital epiblepharon, a much more common condition, by the fact that the tarsus is inverted (Fig. 3‑3). This eyelid malposition does not resolve spontaneously and requires surgical intervention to prevent corneal morbidity. It has been postulated that an abnormal insertion of the lower lid retractors is the underlying cause.

3.3 Applied Surgical Anatomy
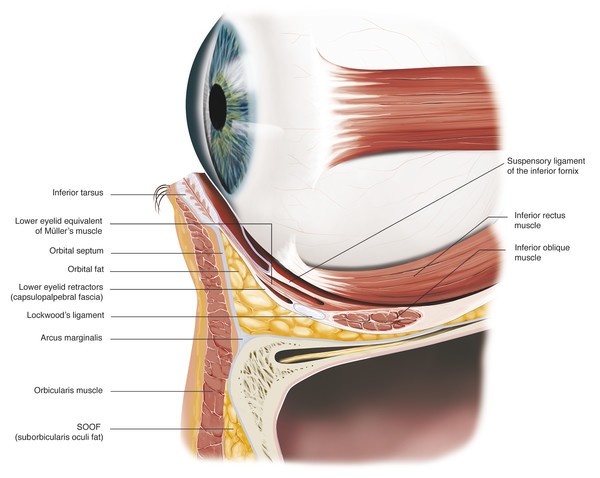
A thorough understanding of lower eyelid anatomy is essential to the surgical management of lower eyelid entropion (Fig. 3‑4). For a more detailed description of the anatomy of the lower eyelid, refer to Chapter 2.
The lower eyelid can be considered to consist of three lamellae:
Anterior: skin and orbicularis oculi muscle.
Middle: orbital septum and inferior eyelid retractors.
Posterior: tarsus and conjunctiva.
The lower eyelid tarsus is approximately 3 to 4 mm in height and 1 mm in thickness. The normal lower eyelid margin is flat, ending at right angles anteriorly and posteriorly. The most posterior aspect of the normal eyelid margin is the mucocutaneous junction where the mucosa of the palpebral conjunctiva ends and the keratinized skin of the eyelid margin begins. The meibomian gland orifices lie just anterior to the mucocutaneous junction. Anterior to the meibomian gland orifices lies the gray line. The gray line is used as a surgical landmark to separate the anterior and posterior lamellae of the eyelid. The eyelashes lie anterior to the gray line. These lie in one or two irregular rows in the lower eyelid and three or four irregular rows in the upper eyelid.
The tarsal conjunctiva is firmly adherent to the tarsus and cannot be dissected freely. The forniceal conjunctiva, in contrast, is very loosely attached to the underlying retractors. The lower eyelid skin crease is variable but usually situated approximately 4 to 5 mm below the eyelid margin. The lateral canthal angle normally sits approximately 2 mm higher than the medial canthal angle.
The lower eyelid retractor complex consists of an aponeurotic expansion from the inferior rectus muscle. This aponeurotic expansion, known as the capsulopalpebral fascia, extends anteriorly to envelop the inferior oblique muscle, where it fuses with the inferior suspensory ligament (Lockwood’s ligament). The fascia also contains fibers that insert into the inferior margin of the tarsus, the preseptal orbicularis muscle at the level of the lower lid skin crease, and the inferior fornix. The fascia is also accompanied by some smooth muscle fibers. The retractors pull the lower eyelid inferiorly on downgaze, acting synchronously with the inferior rectus muscle. Normal tension on the lower eyelid retractors is essential in the maintenance of a stable lower eyelid.
The orbital septum fuses with the fascia approximately 4 to 5 mm below the tarsus. The orbital septum extends from the arcus marginalis of the inferior orbital margin to the inferior border of the tarsus. Posterior to this lie the three lower lid fat pockets.
The anatomy of the lower eyelid resembles that of the upper eyelid. Although the tarsus is much smaller, the capsulopalpebral fascia is analogous to the levator aponeurosis. The smooth muscle fibers accompanying this fascia are analogous to Müller’s muscle. Lockwood’s ligament is analogous to Whitnall’s ligament. The fat in the lower eyelid lies posterior to the septum but anterior to the capsulopalpebral fascia and is analogous to the upper lid preaponeurotic fat. There are three fat pads in the lower eyelid: medial, central, and lateral. These lie between the capsulopalpebral fascia and the orbital septum. The inferior oblique muscle lies between the medial and central fat pads. The central and lateral fat pads are separated by the arcuate expansion.
In the lower eyelid, an anastomotic arterial arcade runs in the orbicularis oculi muscle plane approximately 4 to 5 mm below the eyelid margin.
It is very helpful to consider the individual layers of the lower eyelid that are encountered during a surgical dissection. A full-thickness horizontal incision made through the eyelid at a point 4 to 5 mm below the tarsus would pass through the following structures:
Skin.
Orbicularis oculi muscle.
Orbital septum.
Preaponeurotic fat.
Lower eyelid retractors.
Conjunctiva.
Preaponeurotic fat is often encountered a few millimeters inferior to this position, particularly in an elderly patient. The orbital septum is very attenuated in this age group and should be opened more inferiorly to expose the fat. This ensures that the septum has been opened and released and the inferior retractors (the capsulopalpebral fascia) are correctly identified. This lies beneath the fat and above the conjunctiva.
The involutional entropion presents the trainee oculoplastic surgeon with the ideal opportunity to appreciate eyelid anatomy, to improve surgical skill in eyelid dissection, to perfect the use of the Colorado needle and bipolar cautery in achieving good hemostasis, to practice suturing, and to perfect patient communication during surgery with local anesthesia.
3.4 Patient Assessment
3.4.1 History
Patients who present with a lower eyelid entropion complain of irritation, photophobia, and a red eye. Occasionally they will complain of discharge. The patient may experience only intermittent symptoms and may show no physical abnormalities when they present. Such a history in an older patient should lead to the suspicion that an intermittent involutional entropion is the cause of the patient’s complaints. Some patients discover that the eyelid can be manually repositioned, offering temporary relief from the symptoms. Others present with tape placed at the eyelid–cheek junction to prevent the recurrence of the entropion.
Patients with involutional entropion are commonly elderly individuals with multiple medical problems. The patient’s age and medical and drug history must be taken into account when determining the appropriate management. Most elderly, infirm patients are better suited to the placement of simple lower eyelid everting sutures in the clinic. These are quick and simple to place, very effective, and easy to repeat in the event of a recurrence of the entropion. In the presence of significant lower eyelid laxity, transverse sutures can be used instead, because everting sutures can lead to a secondary ectropion in patients with such a degree of eyelid laxity.
Key Point
Many patients presenting with an involutional lower eyelid entropion are elderly with systemic comorbidities. Such patients are better suited to the placement of simple lower eyelid everting sutures.
3.4.2 Examination
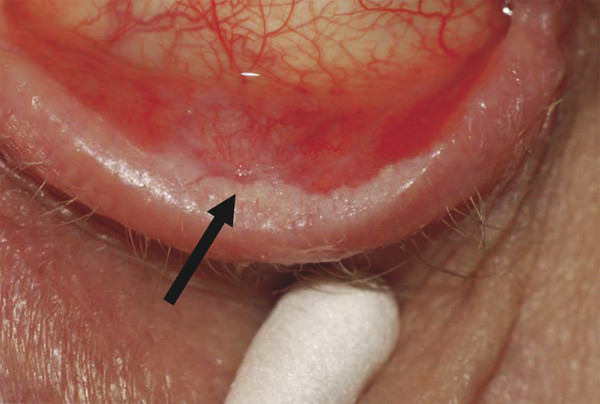
The patient should undergo a careful naked eye and slit-lamp examination to determine the cause of the entropion (e.g., a corneal foreign body causing a spastic entropion) and to determine the most appropriate treatment. The conjunctiva is examined to exclude scarring, symblepharon, or keratin on the posterior lamella (Fig. 3‑5).
The lower lid is gently repositioned with a finger. If the eyelid remains in a normal position without blinking, the cause is likely to be involutional rather than cicatricial, although more than one causative factor may be present. If no entropion is present but the history suggests an intermittent episodic inversion of the eyelid, the patient should be asked to look down and to forcibly close the eyes. The patient should then be asked to slowly open the eyes, and the eyelid should be carefully observed. An entropion may appear or the preseptal orbicularis muscle may be seen to roll upward (overriding of the preseptal orbicularis).
The eyelid margin should be observed in downgaze. Laxity, dehiscence, or disinsertion of the lower eyelid retractors is associated with a poor movement of the eyelid margin when the patient looks down. The eyelid margin is seen to ride above the inferior limbus.
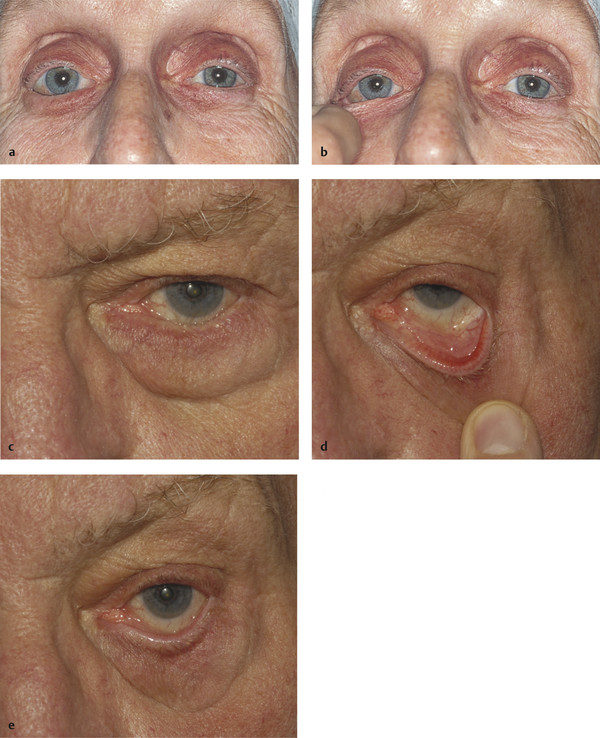
The eyelid should be assessed for horizontal laxity. The eyelid should be drawn medially and laterally to determine the degree of medial and lateral canthal tendon laxity (the “distraction” test). It is unusual to have significant medial canthal tendon laxity in lower lid entropion, and it is extremely rare for this to require surgical correction. This is in contrast to the situation with lower lid ectropion. The eyelid should be drawn away from the globe to determine the degree of laxity of the tarsus. It should only be possible to draw the eyelid approximately 2 to 3 mm from the globe. This is the “pinch” test (Fig. 3‑6a,b). The eyelid is then drawn inferiorly and released. This is the “snap” test (Fig. 3‑6c–e). The eyelid should return to lie in apposition to the globe without a blink. Failure to do so suggests significant eyelid laxity.
3.5 Management
3.5.1 Medical Management
In the case of acute spastic entropion, the treatment is directed to the provoking stimulus (e.g., trichiasis, blepharitis, or a dry eye). Although a bandage contact lens or botulinum toxin injections may improve symptoms temporarily, these are rarely justified. The use of lower lid tape can be advised for use in a primary care setting while the patient is waiting to be seen by an ophthalmologist.
3.5.2 Surgical Management
Involutional Entropion
Although more than 100 procedures have been described for the surgical repair of lower eyelid involutional entropion, very few have withstood the test of time, and most have been abandoned. This is mainly because these procedures have failed to address the underlying factors responsible for the entropion.
Although a multitude of operations are still used by many different surgeons, only those procedures used in my clinical practice are described:
Everting or transverse sutures.
Lower lid retractor advancement with a lateral tarsal strip procedure.
Lower lid retractor advancement with a lower lid wedge resection.
These procedures are usually performed under local anesthesia, with or without sedation.
Everting sutures are offered to all patients older than age 70 years at the initial consultation and are used exclusively for the following patients:
Elderly patients with concomitant medical problems for whom surgery is contraindicated.
Patients who decline a more definitive surgical treatment.
Patients who have a bleeding diathesis or who take anticoagulants.
Patients who are unable to cooperate with more prolonged surgery.
Patients who are unable to lie in a semirecumbent position for the duration of surgery.
Patients willing to undergo a trial of everting sutures.
Everting sutures have been commonly regarded as a temporary form of treatment, but many patients achieve a long-lasting or permanent result with the sutures alone. If the entropion recurs within a relatively short period, the patient is then offered a more definitive surgical procedure unless surgery is contraindicated. The sutures are very quick and simple to insert in a clinic setting and provide instant relief for the patient. It is also very easy to repeat such treatment as required. If the patient has significant eyelid laxity, transverse sutures are placed rather than everting sutures to avoid the possibility of causing a secondary ectropion. For some patients with lower lid laxity, everting sutures can be combined with a lateral tarsal strip procedure.
Key Point
Lower lid everting sutures are very quick and simple to place and have a high success rate. They can be used as the definitive treatment of a lower lid entropion in an older patient, or they can be used as a trial treatment before considering a more invasive procedure.
For all other patients, a lower eyelid retractor advancement is combined with either a lateral tarsal strip procedure or, less commonly, a lower eyelid wedge resection. Wherever appropriate these procedures can be combined with a debulking of the orbicularis oculi muscle—for example, in a patient who has very marked orbicularis hypertrophy or overaction, or with a lower eyelid blepharoplasty (e.g., in a patient with marked fat pad prolapses and/or marked skin laxity).
Key Point
If a retractor advancement is not combined with a horizontal eyelid tightening procedure, the potential for recurrence of the entropion is high, even if the degree of lower eyelid laxity is not considered significant.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


