8 The Management of Thyroid-Related Eyelid Retraction
Abstract
“The Management of Thyroid-Related Eyelid Retraction” addresses this phenomenon in Graves’ disease. The appropriate management of this condition depends on an understanding of the pathophysiological mechanisms responsible for the eyelid malposition. Attention to the pathophysiology of the eyelid malposition permits the selection of the most appropriate intervention and improves the predictability of the outcome. Several different mechanisms may occur singly or in combination and with varying degrees of asymmetry. Surgery to manage eyelid retraction in thyroid eye disease should be deferred until the disease has entered a quiescent phase, unless exposure keratopathy unresponsive to medical therapy requires more urgent intervention. Eyelid retraction surgery undertaken during the active phase can compromise the outcome. In general, the thyroid status and eyelid position should be stable for a minimum period of 6 months before any eyelid surgery is undertaken.
8.1 Introduction
The appropriate management of eyelid retraction in Graves’ disease depends on an understanding of the pathophysiological mechanisms responsible for the eyelid malposition. Attention to the pathophysiology of the eyelid malposition permits the selection of the most appropriate intervention and improves the predictability of the outcome. In the upper and lower eyelids the pathophysiological mechanisms are as follows:
Adrenergic stimulation of Müller’s muscle and its smooth muscle equivalent in the lower eyelid.
Pseudoproptosis caused by axial myopia.
Proptosis.
Inflammation and fibrosis of the upper and lower eyelid retractors.
Inflammation and fibrosis of the anterior orbital fascial septa.
Fibrosis of the tensor intermuscularis.
Inflammation and fibrosis of the inferior rectus muscle.
These mechanisms may occur singly or in combination and with varying degrees of asymmetry.
Mild degrees of eyelid retraction caused by increased sensitivity of Müller’s muscle and its smooth muscle equivalent in the lower eyelid to circulating catecholamines may resolve with treatment of the hyperthyroid state.
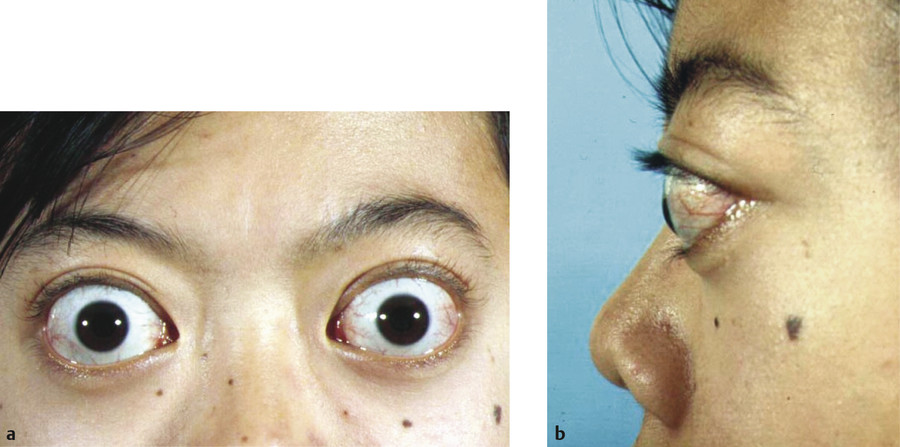
Axial myopia is commonly overlooked as a cause of eyelid retraction. High myopia can compound other mechanisms of eyelid retraction and make the surgical management particularly challenging (Fig. 8‑1).
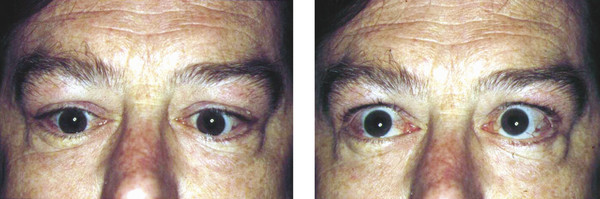
Proptosis, similarly, acts as a wedge between the eyelids. In many patients, treatment of the proptosis by orbital decompression surgery can relieve the eyelid retraction, particularly lower eyelid retraction (Fig. 8‑2), but eyelid retraction will only improve in those patients in whom proptosis is the major cause of the retraction.

Inflammation and fibrosis of the upper and lower eyelid retractors can be responsible for marked degrees of eyelid retraction (Fig. 8‑3). Downward traction applied by the examiner to the upper eyelid margin will be met with marked resistance.

Inflammation and fibrosis of the anterior orbital fascial septa also play a part in eyelid retraction in some patients. This is evident at surgery, when lid retraction may persist despite a satisfactory degree of eyelid retractor recession having been achieved.
Fibrosis of the tensor intermuscularis, the muscle fibers lying circumferentially within the superolateral intermuscular septum, may account for the disproportionate lateral lid retraction seen in Graves’ disease.
Inflammation and fibrosis of the inferior rectus muscle may cause a hypotropia with a compensatory overaction of the superior rectus–levator complex, causing eyelid retraction. The degree of eyelid retraction should be assessed and compared in downgaze and upgaze. Upper eyelid retraction that worsens on upgaze is caused by fibrosis of the inferior rectus muscle (Fig. 8‑4). Such patients also demonstrate a rise in intraocular pressure on upgaze. A recession of the inferior rectus muscle with adjustable sutures should be considered for such patients and should be undertaken after an orbital decompression procedure but before any eyelid lengthening procedure. An inferior rectus recession can cause an increase in proptosis and can result in worsening of lower eyelid retraction.
8.2 Patient Evaluation
The patient should be carefully evaluated to determine the following:
The degree of activity of the disease.
The mechanisms responsible for the eyelid retraction.
The severity of any exposure keratopathy.
The degree of eyelid retraction.
The variability of the eyelid retraction.
The patient’s upper eyelid margin and eyelashes should be grasped between the examiner’s forefinger and thumb and downward traction applied. The degree of resistance should be noted. Marked resistance is indicative of fibrosis within the upper lid retractors, the anterior orbital fascial septa, and/or the tensor intermuscularis. Surgery on such patients will be more difficult and will have a less predictable outcome.
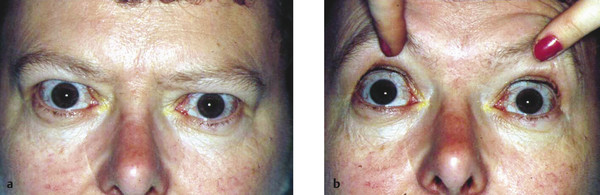
In some patients the degree of upper eyelid retraction can be underestimated because of the presence of a brow ptosis and dermatochalasis or upper eyelid swelling. The brows should be gently elevated to ascertain the true position of the upper eyelids (Fig. 8‑5).
8.3 Timing of Surgical Intervention
Surgery to manage eyelid retraction in thyroid eye disease should be deferred until the disease has entered a quiescent phase, unless exposure keratopathy unresponsive to medical therapy requires more urgent intervention. Eyelid retraction surgery undertaken during the active phase can compromise the outcome. In general, the thyroid status and eyelid position should be stable for a minimum period of 6 months before any eyelid surgery is undertaken. When such surgery has to be postponed because of active thyroid eye disease, chemodenervation-induced ptosis using botulinum toxin injections can be considered (10–20 units of Dysport/Azzalure can be injected subconjunctivally into Müller’s muscle just above the tarsus, or transcutaneously into the levator muscle, and repeated as required after 10 days), or a temporary lateral tarsorrhaphy can be performed.
Key Point
As a general rule, eyelid surgery should be undertaken after orbital decompression surgery and any strabismus surgery, should these be required.
8.4 Orbital Decompression Versus Eyelid Surgery
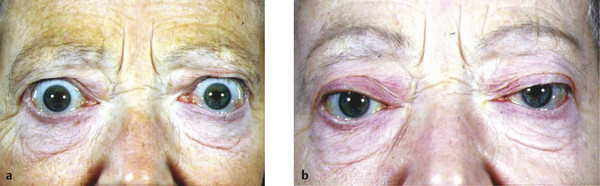
It can be difficult to counsel a patient with significant proptosis about the relative merits of orbital decompression surgery versus eyelid repositioning surgery in the absence of other clear indications for orbital decompression, such as compressive optic neuropathy unresponsive to medical therapy. In the presence of a significant degree of proptosis, unilateral proptosis or asymmetrical proptosis, there is no question that eyelid repositioning surgery alone will not achieve a good cosmetic result for the patient (Fig. 8‑6). Orbital decompression surgery is, however, far more invasive than eyelid surgery alone and is associated with a number of risks such as visual loss and diplopia. The decision should be made on an individual basis.
A patient must be carefully counseled about the aims, risks, and potential complications of surgery. Unrealistic expectations will lead to an unhappy patient postoperatively. The patient should be prepared for the possibility of multiple surgical procedures to achieve the desired end result. Many patients also seek blepharoplasty surgery hoping to restore their appearance to that which preceded the onset of their thyroid eye disease. Such patients should understand that this is rarely achieved and that infiltration of the eyelid by glycosaminoglycans with sub-brow soft tissue thickening is not amenable to complete surgical correction. They also need to appreciate that an upper lid blepharoplasty runs the risk of postoperative lagophthalmos or an incomplete blink with exacerbation of any preexisting dry eye problems.
8.5 Upper Eyelid Retraction
The upper eyelid, in contrast to the lower eyelid, does not require the use of spacer grafts to achieve the desired postoperative eyelid position.
8.5.1 Methods of Upper Eyelid Lowering
A variety of surgical procedures have been described to manage upper eyelid retraction in Graves’ disease. All these procedures aim to reduce upper eyelid retractor tone. The choice of procedure depends on the degree of eyelid retraction and the degree of resistance to downward traction of the upper eyelid. The aim is to achieve a satisfactory lowering of the eyelid without a temporal flare, which can adversely affect the cosmetic result. I use several procedures:
Müllerectomy (1–2 mm of retraction).
Posterior-approach levator recession and Müllerectomy (2–3 mm of retraction).
Posterior-approach levator recession with partial division of lateral levator horn and Müllerectomy (2–3 mm of retraction).
Anterior-approach levator recession with division of lateral levator horn and Müllerectomy (3–4 mm of retraction).
Anterior-approach Z-myotomy with division of the lateral levator horn and Müllerectomy (>4 mm of retraction).
Graded full-thickness blepharotomy.
Müllerectomy
A Müllerectomy is a relatively simple surgical procedure that is useful for small degrees of eyelid retraction (1–2 mm). It can be performed under local anesthesia with or without intravenous sedation or under general anesthesia, because no intraoperative patient cooperation is required to adjust the height or contour of the eyelid.
Surgical Procedure
Between 1 and 1.5 mL of 0.5% bupivacaine with 1:200,000 units of adrenaline mixed 50:50 with 2% lidocaine with 1:80,000 units of adrenaline is injected subcutaneously into the upper eyelid.
A 4/0 silk suture is placed through the gray line of the upper eyelid and the eyelid is everted over a medium Desmarres retractor. The silk suture is fixated to the surgical drapes around the patient’s forehead using a small curved artery clip.
A further 1 mL of local anesthetic solution is injected subconjunctivally. The retractor is removed and pressure is applied for 5 minutes.
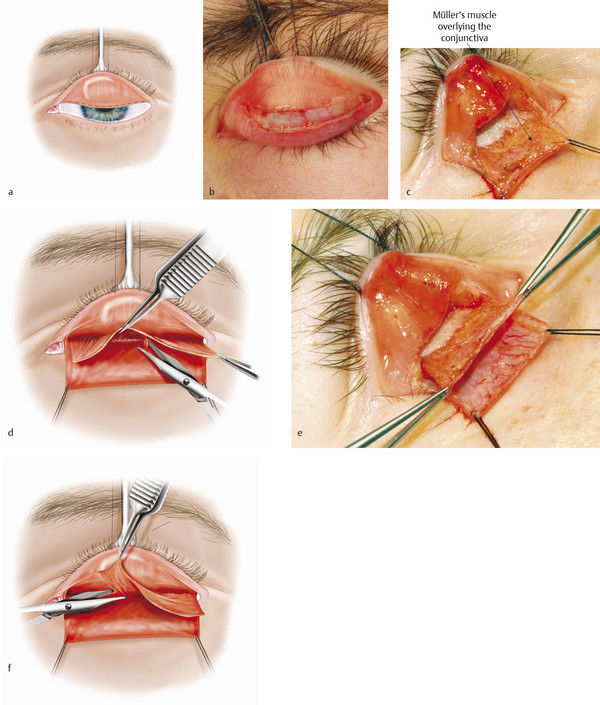
A conjunctival incision is made using a no. 15 Bard Parker blade across the whole of the upper eyelid just above the upper border of the tarsus (Fig. 8‑7a).
The conjunctival edge is lifted with Paufique forceps, and the underlying Müller’s muscle is opened with blunt-tipped Westcott scissors. The surgical space between the levator aponeurosis and Müller’s muscle is dissected open with the Westcott scissors for a distance of approximately 10 to 12 mm. Müller’s muscle will contain fatty tissue and will bleed (Fig. 8‑7b). Bipolar cautery will be required frequently, with the surgeon taking great care to protect the cornea from any damage from the cautery.
Sutures of 4–0 silk traction are passed through the medial and lateral edges of the conjunctiva with a double pass, and the sutures are fixated to the face drapes with small curved artery clips, ensuring that the sutures are drawn medially and laterally away from the cornea.
Between 0.5 and 1.0 mL of local anesthetic solution is carefully injected into Müller’s muscle with the eye protected and left to work for a few minutes. A cotton-tipped applicator moistened with saline can be slipped under the conjunctiva and used both to lift the tissue and to protect the eye as the injection is undertaken.
An incision is then made through Müller’s muscle close to the traction sutures using blunt-tipped Westcott scissors (Fig. 8‑7c).
Using Castroviejo 0.3-mm toothed forceps and blunt-tipped Westcott scissors, Müller’s muscle is dissected from the underlying conjunctiva with a blunt stripping motion from the cut edge of the conjunctiva to its superior origin from the levator.
Müller’s muscle is excised, leaving a small residual strip nasally to avoid a medial ptosis (Fig. 8‑7d).
The traction sutures are then removed.
Sutures for wound closure are unnecessary and risk causing discomfort or a corneal abrasion.
Postoperative Care
Postoperatively the patient is prescribed a topical antibiotic ointment to the eye three times a day for a week. The patient is instructed to keep the head of the bed elevated for 4 weeks and to avoid lifting any heavy weights for 2 weeks. The patient should be evaluated in the office within a week and the antibiotic ointment discontinued and antibiotic drops prescribed instead for a further week. If the eyelid begins to rise above the desired position, the patient should be instructed to commence eyelid traction to maintain the desired height and contour of the upper eyelid. The patient should grasp the edge of the eyelid and lashes at the peak of the eyelid while looking down, and should then pull the eyelid down firmly while looking up. This can be continued for 2 to 3 minutes three times a day for a period of 4 to 6 weeks.
Posterior-Approach Levator Recession with Müllerectomy
This approach can be performed under local anesthesia with intraoperative monitoring of the eyelid position, with or without intravenous sedation as required.
Advantages
No sutures are required.
The height and contour of the eyelid can be manipulated postoperatively with eyelid traction.
The absence of a skin incision reduces the degree of postoperative eyelid edema and permits a more rapid postoperative recovery.
The absence of an incision through the orbicularis muscle avoids temporary denervation of the orbicularis muscle and secondary lagophthalmos.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


