6 Lower Eyelid Ectropion
Abstract
“Lower Eyelid Ectropion” discusses an eyelid malposition in which the lower eyelid margin is turned away from its normal apposition to the eyeball. It is more common than upper eyelid ectropion. The condition may be due to involutional changes (the most common cause) with advancing age or a pathology such as Ehlers–Danlos syndrome; scarring; displacement of the eyelid by a mass lesion or other mechanical cause; or a facial nerve palsy. More than one of these etiological factors may be present in an individual patient. It is important to be able to classify the type of ectropion that is seen so that the correct treatment is directed at the underlying cause. Failure to recognize this leads to poor results from inappropriately selected surgical procedures. This chapter describes all surgical procedures and postoperative care in each instance in detail.
6.1 Introduction
Eyelid ectropion is an eyelid malposition in which the eyelid margin is turned away from its normal apposition to the globe. This more commonly affects the lower eyelid. Upper eyelid ectropion is more unusual. The condition may be classified into four categories according to the underlying etiology.
6.2 Classification
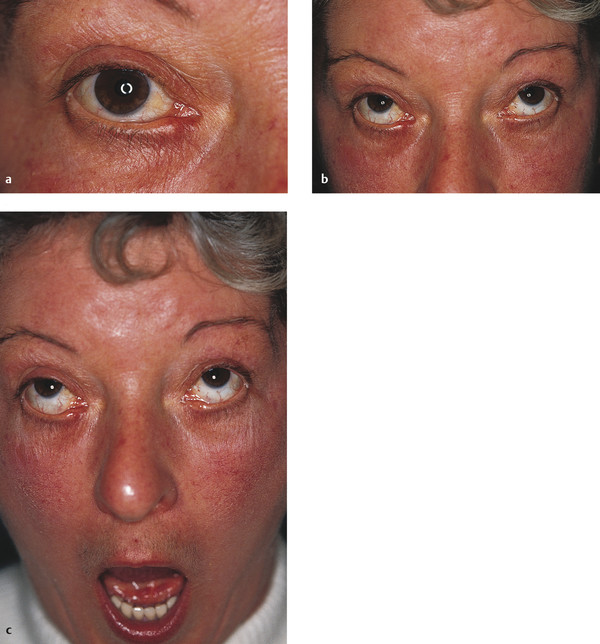
Involutional ectropion (Fig. 6‑1a)
Cicatricial ectropion (Fig. 6‑1b)
Paralytic ectropion (Fig. 6‑1c)
Mechanical ectropion (Fig. 6‑1d)
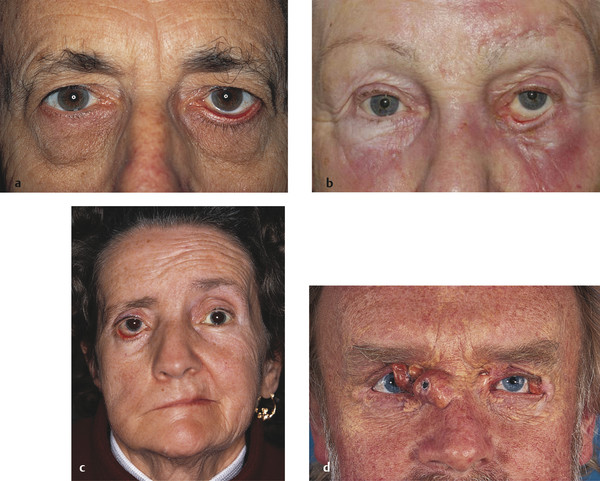
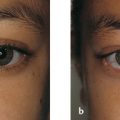
It should be recognized, however, that more than one etiological factor may be present in an individual patient; for example, in a patient with a chronic facial palsy and a lower lid ectropion, all four etiological factors may coexist (Fig. 6‑2a). An ectropion affecting the upper eyelid is less commonly encountered and may occur after eyelid trauma, herpes zoster ophthalmicus, ichthyosis, and burns (Fig. 6‑2b).

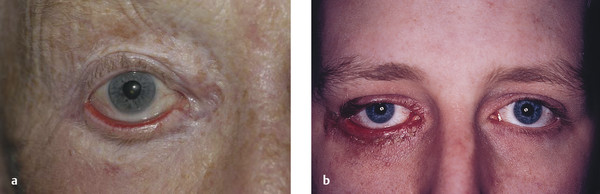
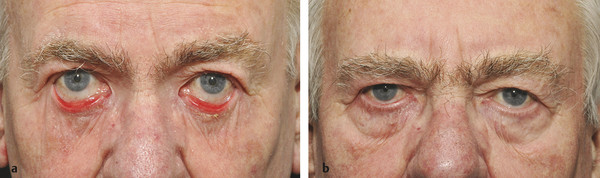
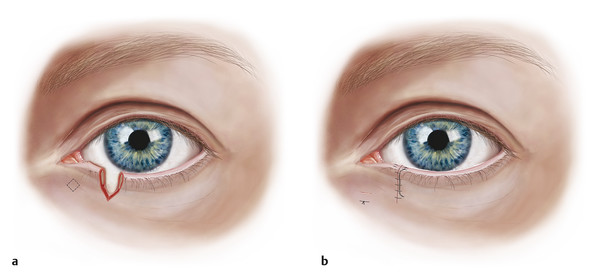
It is important to be able to classify the type of ectropion that is seen so that the correct treatment is directed at the underlying cause. Involutional ectropion is by far the most common type of ectropion, but a cicatricial cause of lower lid ectropion is often overlooked (Fig. 6‑3a). Such an ectropion will only respond to the addition or recruitment of skin into the lower eyelid using a full-thickness skin graft, a local skin flap, a midface lift, or soft tissue expansion. Failure to recognize this leads to poor results from inappropriately selected surgical procedures (Fig. 6‑3b).
Key Point
A cicatricial cause of lower lid ectropion should not be overlooked.
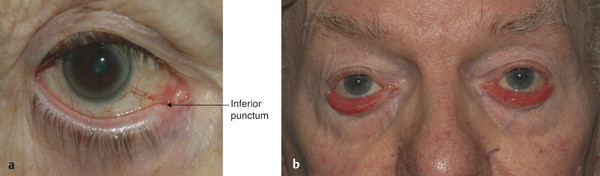
The initial sign of a lower lid ectropion is inferior punctal eversion (Fig. 6‑4a). This can lead to a vicious cycle of secondary events and needs to be addressed early. Eversion of the inferior punctum leads to exposure and drying of the punctum, which becomes stenosed. Epiphora ensues, which may lead to excoriation and contracture of the skin of the lower eyelid that further exacerbates the ectropion. In addition, the patient tends to continually wipe the tears from the lower eyelid, which in turn results in eyelid and medial canthal tendon laxity that further exacerbates the lower eyelid ectropion. If the condition is neglected, the tarsal conjunctiva becomes exposed and eventually thickened and keratinized (Fig. 6‑4b). Lower lid ectropion often results in a corneal epitheliopathy, especially in the inferior third of the cornea.
6.3 Patient Evaluation
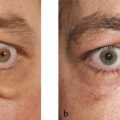
The patient’s history may point to a number of dermatological disorders that may be responsible for a cicatricial ectropion, such as eczema, lamellar ichthyosis, contact or allergic dermatitis (Fig. 6‑5a). A drug history may reveal topical medications the patient may be taking to which there may be an allergy with a secondary chronic dermatitis, such as topical glaucoma medications (Fig. 6‑5b). This is not an uncommon cause of lower lid ectropion in elderly patients attending glaucoma clinics and is often overlooked or misdiagnosed.

Patients who have previously undergone a lower eyelid transcutaneous blepharoplasty, laser skin resurfacing, or a chemical peel may be reluctant to divulge such information. A lower lid ectropion can affect a patient many years after a lower lid transcutaneous blepharoplasty, and the patient may not appreciate any causative link (Fig. 6‑6).
Key Point
A chronic contact or allergic dermatitis is not an uncommon cause of a lower lid ectropion in elderly patients attending glaucoma clinics and is often overlooked or misdiagnosed.
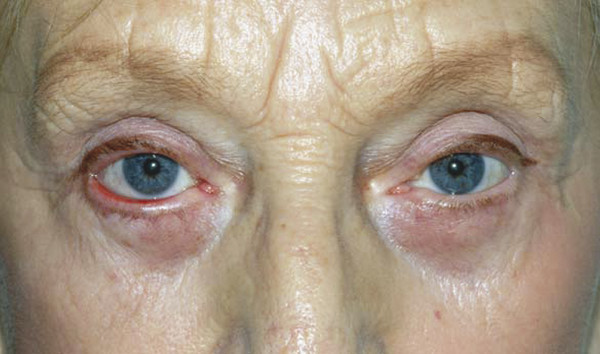
When examining the patient, the whole of the patient’s face should be scrutinized for evidence of a dermatological disorder, connective tissue disorder, facial weakness, scars from previous surgery or trauma, or evidence of malignant cutaneous lesions (Fig. 6‑7). The degree of eyelid laxity is assessed by drawing the eyelid down and away from the globe and releasing it (the “snap” test) (Fig. 6‑8).


The distance that the lid can be pulled away from the globe using the thumb and forefinger can also be measured in millimeters using a ruler (the “pinch” test).
The eyelid is drawn laterally, and the position of the punctum is observed (the “lateral distraction” test). If the punctum can be drawn lateral to the medial limbus with the globe in the primary position, the medial canthal tendon will probably require attention during the surgical repair of the ectropion (Fig. 6‑9). Rounding of the lateral canthus indicates lateral canthal tendon laxity or dehiscence.

If a cicatricial component of the ectropion is not obvious, the lower eyelid skin should be observed for tension lines seen when the patient blinks. The patient is asked to look up and to open the mouth to determine whether these maneuvers exacerbate the ectropion (Fig. 6‑10).
Key Point
Failure to recognize a cicatricial component is a common cause of surgical failure in the management of lower lid ectropion.
6.4 Management
It is important to recognize dermatological causes of cicatricial ectropion that may be amenable to medical management alone, such as chronic allergic or contact dermatitis or severe eczema (Fig. 6‑11).
Removal of the offending substance, such as replacement of a topical glaucoma medication with a preservative-free preparation along with a short course of a weak topical steroid cream to the eyelid skin, may be all that is required.
The choice of surgical procedure depends on a number of factors:
The degree of ectropion.
The location of the ectropion.
The degree of laxity of the medial and lateral canthal tendons.
The horizontal laxity of the eyelid.
The tone of the orbicularis muscle.
The nature of any cicatricial forces.
The presence of any mechanical force.
The age and general health of the patient.
The surgical procedures should be selected to address these factors in each individual patient. Although an abundance of surgical procedures has been described for the management of lower eyelid ectropion, the choice of procedure can in practice be made from a relatively small number for the management of most patients. I use the following procedures:
Retropunctal cautery.
Medial spindle.
Medial spindle with medial wedge resection.
Medial canthal tendon plication.
Medial canthal resection.
Lateral wedge resection.
Lateral wedge resection with skin–muscle blepharoplasty.
Lateral tarsal strip procedure.
Z-plasty.
Lateral wedge resection or lateral tarsal strip with skin graft.
Posterior approach retractor reinsertion with medial spindle with lateral tarsal strip.
Fascia lata sling.
Removal of lesion causing mechanical ectropion.
Local tissue flap.
Midface lift.
Soft tissue expansion with local tissue flap.
6.4.1 Involutional Ectropion
Involutional ectropion can be further classified into the following subtypes:
Punctal ectropion.
Medial ectropion without horizontal eyelid laxity.
Medial ectropion with horizontal eyelid laxity.
Medial ectropion with medial canthal tendon laxity.
Ectropion of the whole length of the lower eyelid.
Complete tarsal ectropion.
Punctal Ectropion
In the initial stages of lower lid ectropion, it is simple to apply retropunctal cautery to reposition the everted punctum.
Retropunctual Cautery
Surgical Procedure
One to two milliliters of 2% lidocaine with 1:80,000 units of adrenaline are injected subcutaneously and subconjunctivally into the medial aspect of the lower eyelid.
Using a disposable cautery device, deep burns are applied to the conjunctiva 3 to 4 mm below the punctum. The effect on the punctal position is observed and titrated by the number of burns applied and the depth of the burn. Great care should be taken when using such a device close to the globe, and inflammable swabs should be kept away from the surgical field.
Antibiotic ointment is instilled into the eye.
Postoperative Care
Antibiotic drops are instilled into the eye three times per day for a week.
Medial Ectropion Without Horizontal Eyelid Laxity
If the punctal ectropion is more pronounced, a medial spindle procedure is performed. It is usually necessary to dilate the punctum with a Nettleship dilator at the same time, because this is often stenosed. It is not usually appropriate to perform any destructive procedures on the punctum (e.g., a three-snip punctoplasty), because the punctum may resume its normal appearance and function once it has been repositioned against the globe. Alternatively, a perforated punctal plug or a Crawford bicanalicular or monocanalicular stent can be placed temporarily to maintain patency of the punctum. If a stenosed punctum needs to be surgically enlarged, it is preferable to do so using a Kelly glaucoma punch.
Medial Spindle
Surgical Procedure
One to two milliliters of 2% lidocaine with 1:80,000 units of adrenaline are injected subcutaneously and subconjunctivally into the medial aspect of the lower eyelid.
A 00 Bowman probe is inserted into the inferior canaliculus. This step is omitted when sufficient surgical experience has been gained.
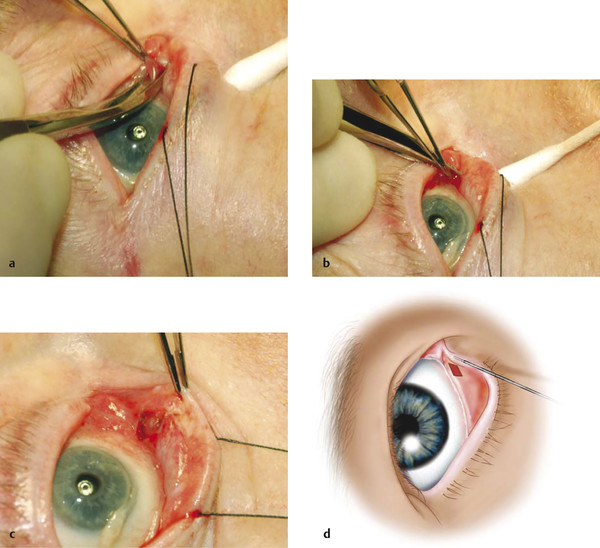
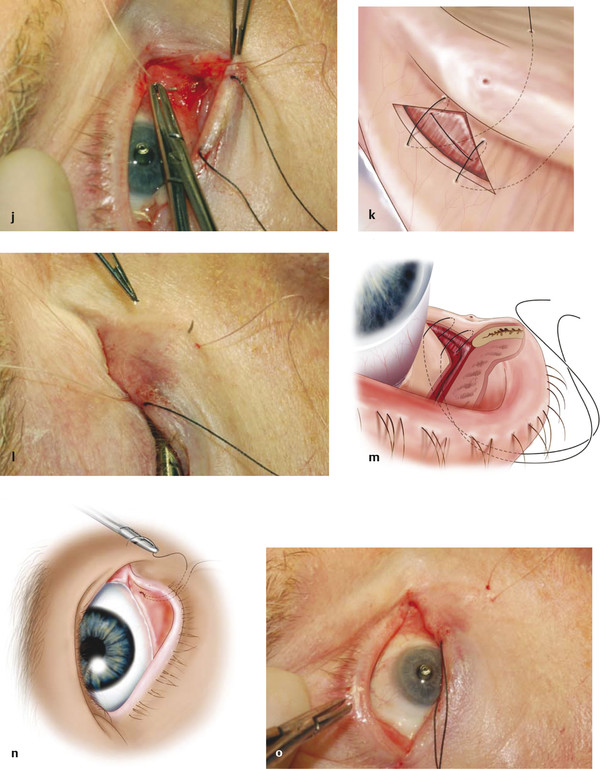
The conjunctiva is lifted just below the inferior punctum using Paufique forceps. A diamond-shaped excision of conjunctiva is performed using Westcott scissors. A cut is made through the tented conjunctiva in a horizontal plane medial and then lateral to the forceps, creating a diamond-shaped excision (Fig. 6‑12a–d).
A double-armed 5–0 Vicryl suture on a quarter-circle needle is passed through the lower eyelid retractors at the base of the conjunctival wound, with the needle rotated toward the globe.
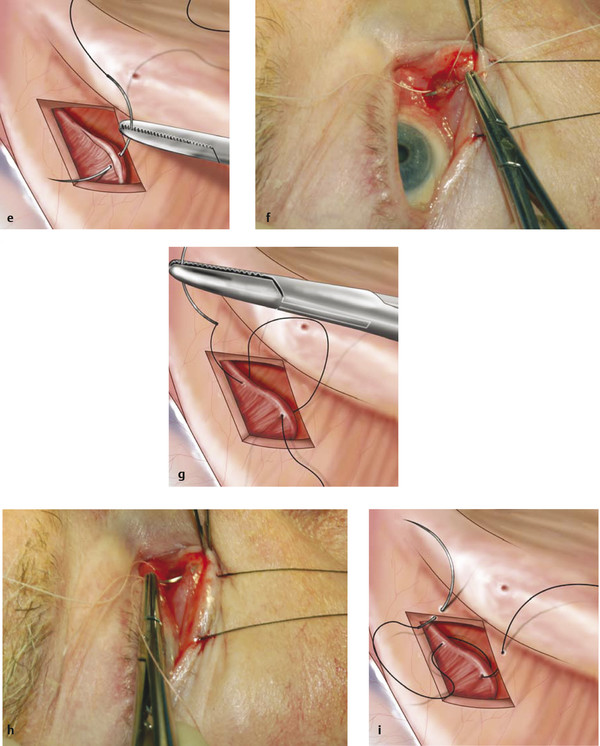
The needle is then reverse mounted and passed away from the globe through the superior edges of the conjunctival wound on either side of the apex of the diamond.
Again the needle is reverse mounted and is then passed back through the inferior edges of the conjunctival wound on either side of the apex of the diamond and out through the skin of the lower lid at the junction of eyelid and cheek skin (Fig. 6‑12e–o). The effect of the suture is to attach the inferior retractors to the superior aspect of the wound, to pull the punctum posteriorly against the globe, and to close the wound. The tension on the suture is titrated against the effect on the position of the punctum. Ideally the punctum should be slightly overinverted against the globe. See Video 6.3.
Postoperative Care
Postoperatively topical antibiotic ointment is prescribed three times a day for 2 weeks, and the patient is instructed not to pull the eyelid down to instill it. The ointment should simply be smeared across the medial aspect of the eyelid. The suture should be removed in the office after 2 to 3 weeks.
Medial Ectropion with Horizontal Eyelid Laxity
For medial ectropion with horizontal eyelid laxity, a medial spindle procedure is combined with a medial wedge resection of the lower eyelid (Fig. 6‑13). The wedge resection is positioned to remove thickened keratinized conjunctiva. It is important that sufficient eyelid is left medial to the resection to enable vertical mattress sutures to be placed across the eyelid margin without risking damage to the punctum or to the inferior canaliculus.
Medial Spindle and Medial Lower Lid Wedge
Surgical Procedure
One to two milliliters of 2% lidocaine with 1:80,000 units of adrenaline are injected subcutaneously and subconjunctivally into the medial aspect of the lower eyelid.
The medial spindle procedure is performed first, but the suture is not tied until the wedge resection has been performed.
The eyelid margin is held with Paufique forceps, and a vertical incision is made with a no. 15 Bard Parker blade through the eyelid margin to a depth of approximately 2 mm. The blade is passed away from the globe for safety.
A vertical incision is then made to the base of the tarsus using straight iris scissors.
Hemostasis is achieved using bipolar cautery.
A second pair of Paufique forceps is then used to overlap the medial and lateral edges of the cut eyelid to assess the amount of eyelid that can safely be removed without placing undue tension on the wound.
The eyelid margin is again held with Paufique forceps, and another vertical incision is made with the no. 15 Bard Parker blade through the eyelid margin at the point of overlap.
A vertical incision is then made to the base of the tarsus using straight iris scissors.
The wedge excision is completed by angling the iris scissors 45 degrees at the base of the eyelid wounds and cutting inferomedially and inferolaterally.
A 5–0 Vicryl suture on a half circle needle is then passed through the tarsus just below the eyelid margin, ensuring that the suture lies above the surface of the conjunctiva posteriorly and just beneath the skin anteriorly. The suture is tied with a single throw and the alignment of the eyelid checked. If it is not satisfactory, the suture is replaced. Once the alignment is satisfactory, the suture is loosened and used for traction by fixating it to the head drape using an artery clip. This elongates the wound, making it easier to place further sutures in the tarsus.
Further 5–0 Vicryl sutures are placed horizontally through the tarsus and orbicularis muscle below the tarsus and tied.
The initial suture is tied.
A 6–0 black silk suture is passed horizontally through the gray line 2 to 3 mm from the wound edge and brought out through the gray line a similar distance from the wound edge. The needle is then reverse mounted and passed back as a horizontal mattress suture through the wound edges. The suture is tied, causing the wound edges to evert slightly. A further 6–0 black silk suture is passed in the same way through the lash line and tied. The suture ends are cut but left long. The ends are incorporated in the skin closure sutures to keep the suture ends away from the cornea.
The skin edges are closed with interrupted 7–0 Vicryl sutures or with 6–0 black silk sutures.
Antibiotic ointment is instilled into the eye.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


