29 Traumatic Optic Neuropathy
Abstract
“Traumatic Optic Neuropathy” discusses injuries to the optic nerve, which are rare and may result from a variety of mechanisms. Direct injury to the optic nerve can be caused by penetrating orbital trauma, partial or complete avulsion, or an intraoptic nerve sheath hematoma. Indirect injury to the optic nerve can result from an optic canal fracture with contusion of the optic nerve or edema within the optic canal after a blow to the supraorbital area, or from an expanding intraorbital hematoma. Evaluation of the patient may be difficult, especially if the patient is unconscious. It is extremely important to exclude other causes of visual loss. Orbital decompression by immediate lateral canthotomy and inferior cantholysis, if indicated (e.g., in acute orbital compartment syndrome related to the development of a retrobulbar hematoma), must not wait for imaging studies. The treatment for posterior indirect traumatic optic neuropathy is determined on an individual basis.
29.1 Introduction
Injuries to the optic nerve are rare and may result from a variety of mechanisms:
Direct injury to the optic nerve.
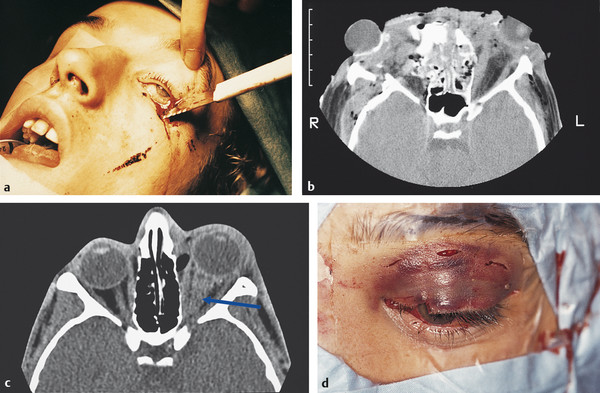
Penetrating orbital trauma (Fig. 29‑1a).
Partial or complete avulsion (Fig. 29‑1b).
Intraoptic nerve sheath hematoma (Fig. 29‑1c,d).
Indirect injury to the optic nerve.
Optic canal fracture with contusion of the optic nerve or edema within the optic canal after a blow to the supraorbital area.
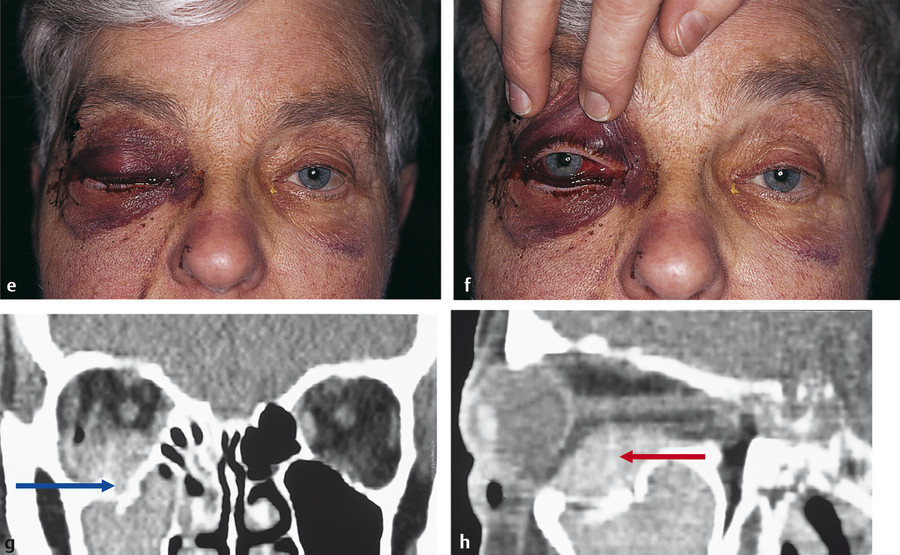
Expanding intraorbital hematoma (Fig. 29‑1e–h).
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


