27 Zygomatic Complex Fractures
Abstract
“Zygomatic Complex Fractures” describes traumatic displacement of the zygoma in what is often referred to as a tripod or tripartite fracture because it usually involves three areas of dislocation: the area of the frontozygomatic suture, the zygomaticomaxillary suture, and the zygomatic arch. Zygomatic fractures usually occur after direct blunt trauma to the cheek. A sign of a zygomatic fracture is a flattening of the malar eminence, but it may be masked by edema. The displaced zygomatic bone may impinge on the coronoid process of the mandible and the temporalis muscle, causing trismus when the patient attempts to open the mouth. The patient can be managed conservatively if the fracture is minor, with little displacement of the zygoma. Otherwise, two surgical approaches are in use: Gillies’ temporal approach and the direct open approach.
27.1 Introduction
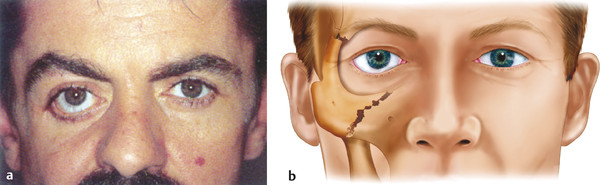
A zygomatic complex fracture refers to a traumatic displacement of the zygoma and is often referred to as a tripod or tripartite fracture. This usually involves three areas of dislocation: the area of the frontozygomatic suture, the zygomaticomaxillary suture, and the zygomatic arch (Fig. 27‑1).

27.2 Etiology
Zygomatic fractures usually occur after direct blunt trauma to the cheek.
27.3 Diagnosis
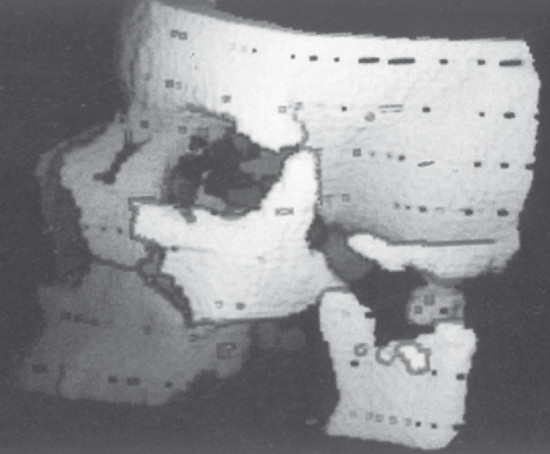
The presence of a zygomatic complex fracture should be suspected in any patient who has sustained blunt trauma to the cheek. The patient should be observed from below, looking for malar flattening. This may, however, be masked by edema. The patient should be asked to open the mouth, looking for trismus. The reason for trismus is demonstrated in the scan seen in Fig. 27‑2. The orbital margin should be carefully palpated for gaps, steps, and areas of tenderness. A neurosensory examination of the area should be performed, because hypoesthesia or anesthesia of the lower eyelid and cheek may be present. Imaging should be performed if there is a clinical suspicion of such a fracture.
27.4 Clinical Signs
The patient should be examined from below. Flattening of the cheek is usually noted (Fig. 27‑3).
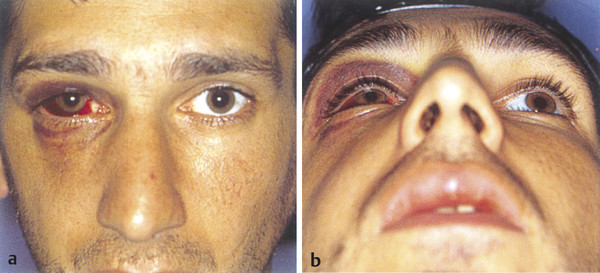
Palpation of the inferior orbital margin may reveal gaps or steps. The signs and symptoms of such a fracture depend on the degree of displacement of the zygoma and the direction of the displacement. The lower eyelid may be dragged inferiorly, the lateral canthus may be displaced inferiorly, or there may be a bulge in the lateral cheek area (Fig. 27‑4).
There is usually an associated orbital floor fracture with enophthalmos, but rarely signs of soft tissue entrapment. The fracture may be associated with other fractures, such as inferior orbital rim fractures.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


