26 Brachioplasty
INDICATIONS
Massive weight loss, such as following bariatric surgery
Skin laxity exceeds subcutaneous fat in the upper arm and possibly lateral chest regions
INTRODUCTION
Brachioplasty is a surgical procedure performed on individuals with excess skin laxity in the upper arm and may include the lateral chest area. 1 – 4 These deformities often cannot be smoothed and toned by diet and exercise alone. A common candidate for this operation is someone who has recently lost a great deal of weight, for example, a patient with massive weight loss after gastric bypass. 1 – 5 As a result, the upper arms have an overabundance of skin. Liposuction alone removes fat but does not tighten the excessive skin; this often results in skin irregularities and deformities. A brachioplasty is designed to remove both the excess skin and the subcutaneous fat. 4 Although the patient is left with a rather long scar, there are benefits to this surgery, including improved self-esteem and increased ease of dressing, and the scar itself may be hidden so it is minimally visible. 2 However, patients need to be counseled on the risks, benefits, and alternatives of proceeding with brachioplasty. In addition to the usual risks of body-contouring procedures, risk of hypertrophic scarring, lymphedema, seroma, injury to the medial antebrachial cutaneous nerve with resulting pain, paresthesias, or numbness need to be emphasized to the patient. Care must be taken not to excise too much skin so that closure without excessive tension can be performed. Table 26.1 indicates special equipment needed for the procedure.
PREOPERATIVE MARKINGS 2 , 4
The patient is marked in a standing position.
Abduct and adduct each arm to determine the level of the axillary crease.
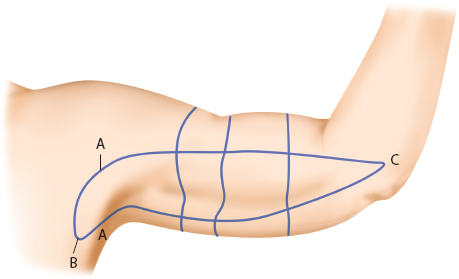
With the patient’s arm abducted at 90° and with the elbow flexed at 90°, pinch along the upper arm to draw a series of anterior and posterior marks.
If redundancy of tissue extends to the axilla and lateral chest, repeat the pinch test along the lateral chest wall along the posterior axillary fold.
These markings are connected to form the outer ellipse (Figure 26.1).
To allow for the distance between the pinching fingers, mark an inner ellipse to allow enough remaining skin to re-approximate following resection.
Make crosshatch marks to help with closure.
Draw a central line through the ellipse to approximate the final scar.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


