22 Correction of prominent ear
INDICATION
Desire to correct prominent ears to achieve symmetric and normal ear aesthetics.
INTRODUCTION
Congenital ear deformities are present in up to 29% of infants, and only one-third of these self-correct. There is a window of opportunity to correct the remaining deformities with ear-molding therapy in the newborn period. The distinction needs to be made between ear deformation, which is amenable to molding, and ear malformation (i.e., microtia), where tissue is deficient and surgical reconstruction is necessary. Ear molding has been shown to be highly successful if initiated within the first week of life. The premise is that circulating maternal estrogen levels are high at birth and the cartilage is most malleable. 1 After 3 weeks of age, molding therapy is successful in fewer than 50% of cases. 2 Table 22.1 indicates equipment needed for the procedure.
Clear adhesive drapes (2) 15 in L ×15 in with circular aperture Clear adhesive drape 10 in × 10 in Bonnie’s blue (or methylene blue) in 1-mL syringe with 27-gauge, 1½-in needle Dressing: Petroleum gauze bacitracin ointment large sterile cotton pad Kerlix roll gauze Flexinet |
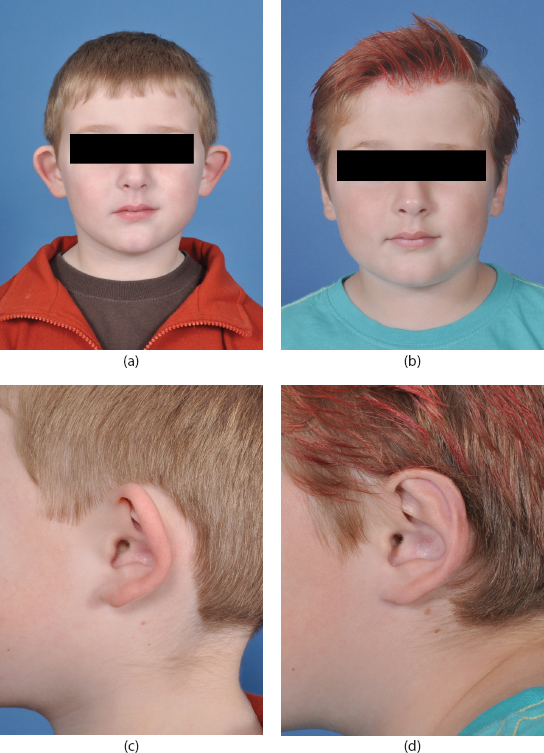
The most common ear deformity is the prominent/cup ear deformity (45%). This may be unilateral or bilateral. Although physiologic effects are minimal, there may be significant psychological distress and emotional trauma associated with the condition. When the older child presents for correction, surgical repair is considered (Figure 22.1a–d).
The goals of surgical otoplasty are as follows 3 :
Correction of all upper third ear protrusion.
The helix of both ears should be visible beyond the antihelix from the anteroposterior (AP) view.
The helix and antihelix should have a smooth contour throughout the entire curve.
The helix-to-mastoid distance should fall within the normal range: 10- to 12-mm upper third, 16-mm middle third, 20- to 22-mm lower third.
The conchoscaphal angle should be 90°.
There should be symmetry within 3 mm between the two ears.
The ear attains nearly 85% of its adult size by age 3 years. Maximum width is reached by approximately age 6 in girls and 7 in boys. 4 Thus, 5–7 years is the optimal timing for surgical correction. As the person matures, the ear cartilage becomes more calcified and stiffer, requiring adaptation of techniques (cartilage breaking rather than molding).
PREOPERATIVE EVALUATION AND DOCUMENTATION
Determine symmetry.
Determine the extent of antihelical folding and conchoscaphal angle.
Note the depth of the conchal bowl.
Evaluate the lobule for prominence and deformity, if present.
Determine the distance between the helical rim and the mastoid plane at the superior, middle, and lower thirds.
Note the flexibility and spring of the auricular cartilage.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


