25 Aesthetic Mandibular Implants
Introduction
The mandible provides a framework for the lower third of the face, and it is most aesthetically pleasing when the chin projects adequately and transitions in a smooth, straight line to the midlateral mandible. A welldefined mandible often conveys an impression of strength, confidence, and assertiveness whereas a weak or hypoplastic mandible can demonstrate the opposite. The aging or hypoplastic mandible generally benefits from chin augmentation—a procedure that commonly complements rhinoplasty and facial rejuvenation surgery.
Initially, years ago, procedures to improve mandibular contour for microgenia focused on the central mentum, where small, centrally located mandibular implants had the negative effect of creating an unnaturally pointed appearance at the chin. In the 1980s, prejowl deficiency was recognized by the primary author to be a contributing factor to the aging process, and extended mandibular implants were created. By 2011, mandibular augmentation procedures were the fastest growing trend in plastic surgery. 1 This operation is extremely gratifying and versatile, as it can improve a mandible affected by age, injury, and congenital deformity, but requires little surgical time and is a rather simple procedure technically. These procedures do not address any functional problems such as malocclusion.
Improved understanding of the anatomy and aging process of the mandible, in addition to the development and improvement of alloplastic implants over the last few decades, has resulted in a wealth of implant designs and materials from which to choose. The authors prefer solid silicone elastomer rubber (Silastic [Dow Corning]) implants due to their ease of use and very low reactivity. These implants are made in different sizes and shapes and are anatomically designed to provide appropriate, natural-appearing augmentation via a rather simple procedure. Additionally, the implants can be replaced easily or removed if a patient is dissatisfied, which is quite uncommon. In contrast, osseous genioplasty requires an osteotomy and plating of the resulting bone fragment, a procedure that is not as easily reversed and with greater morbidity and risk.
The wide array of available implants, as well as the possibility of using injectable filler materials for mandibular augmentation, may seem intimidating; however, a detailed understanding of the mandible, its morphologic variations, and the aging process make the facial plastic surgeon’s choice easier. Overall, a small number of extended mandibular implants can fulfill nearly all of one’s needs. With a properly chosen implant, few operations provide as much benefit in as little time as chin and prejowl groove augmentation. In this chapter, the relevant anatomy, preoperative evaluation, implant selection, and surgical technique are discussed.
Past Medical and Surgical History
All patients interested in cosmetic surgery should be evaluated to ensure that their motivation and psychological state are appropriate. If a significant psychiatric pathology is detected, particularly body dysmorphic disorder, referral for psychiatric services is indicated. One should also screen for bleeding disorders, reactions to anesthesia, osteoporosis, prior radiation treatment, congenital abnormalities, history of trauma to the head and neck, and temporomandibular joint or dental occlusion pathology. Because patients with functional mandibular problems may be candidates for orthognathic surgery rather than chin implantation, referral to an appropriate specialist is indicated in these situations. After gathering a full past medical history, a surgical history should be obtained that includes any cosmetic procedures, both surgical and officebased, such as filler injections. Oftentimes, patients will not discuss critically important prior cosmetic procedures, such as recent filler injection to the chin, unless specifically asked. One should also screen for any past surgery of the head and neck, head and neck trauma reconstruction, surgery for congenital abnormalities, and any dental or orthognathic procedures. If any concerns arise, further specialist referral may be appropriate.
Relevant Anatomy
The mandible is the framework that determines projection of the lower third of the face. It contains the inferior alveolar nerve as well as a number of attachments for the muscles of mastication and facial expression. The inferior alveolar nerve, a branch of the third division of the trigeminal nerve, enters the mandible along its posterior surface at the mandibular foramen and travels through the mandibular canal before exiting anteriorly at the mental foramen, at which point it is known as the mental nerve. The mental nerve then travels superiorly from the foramen to provide sensation to the chin and lower lip on each side. The mental foramen is located at the level of the second mandibular premolar (50%), or just anterior (25%) or posterior (25%) to this location, usually 25 mm from the midline, with a range of 20–30 mm. 2
With age, and especially in edentulous patients, the vertical height of the mandible decreases due to atrophy of the alveolar ridge, leading to an increasingly superior location of the mental foramen. While the distance from the mental foramen to the inferior border of the mandible is relatively constant, there is an often disproportionate atrophy of the inferior border of the mandible at the level of the mental foramen, contributing to a bony and soft tissue deficiency between the jowl and mentum known as the prejowl sulcus. Bony resorption in this location results in some variation of the distance of the mental foramen from the inferior border of the mandible with age. The mental foramen should be located at least 8 mm above the inferior border of the mandible in older adults and at least 10 mm above the inferior border of the mandible in younger adults. On average, however, the mental foramen lies 13 ± 2 mm above the inferior border of the mandible. 3 In childhood, the mental foramen is in a slightly more anterior and inferior position relative to the mandible’s inferior border. 4
There are a number of muscular attachments to the mandible. Several of these muscles adhere to the oblique line, which is a faint ridge of bone that extends from the inferior border of the mandible along its external surface in a posterior and superior direction until reaching the mandible’s superior border at the ramus. Along the oblique line of the mandible lie attachments to the depressor labii inferioris and depressor anguli oris muscles, which course vertically upward to the orbicularis oris, where they depress the lip and corner of the mouth, respectively. The platysma inserts along the mandible’s inferior border anteriorly and just below the oblique line as one moves more posteriorly. The mentalis muscle arises more superiorly at the incisive fossa, approximately 18 ± 3 mm above the inferior border of the mandible, and courses vertically downward to insert on the skin at the mentum. 3 This muscle functions to pull the skin in an upward direction and dimples the chin upon contraction.
The mental foramen superiorly and muscular attachments to the mandible inferiorly define the limits of dissection in which a pocket can be created for placement of a mandibular implant. 3 , 5 In general, the properly designed implant should have a vertical height of 6–8 mm at the level of the mental foramen and, as a rule, should not impinge upon the nerve when placed correctly.
Preoperative Analysis
When evaluating a patient for a mandibular implant, one should first look at the dental occlusion. In normal class I occlusion, the mesiobuccal cusp of the first maxillary molar should lie in the mesiobuccal groove of the first mandibular molar. If this is not the case and there is a symptomatic occlusal problem, the patient may be evaluated for orthognathic surgery. Once the malocclusion has been corrected, persistent mandibular deficiency may be addressed with mandibular augmentation. 6 Patients seeking rhytidectomy or rhinoplasty oftentimes receive significant benefit from concurrent augmentation of the mandible. Importantly, there is no significant difference in complication rates when performing rhytidectomy with mandibular augmentation compared to rhytidectomy alone. 7 Patients considering submentoplasty alone also often benefit significantly from concurrent mandibular augmentation. 8 In addition, another study found that between 17 and 62% of males and 42 and 81% of females seeking rhinoplasty would also benefit from mandibular augmentation. 9 Therefore, the surgeon should pay close attention to the mentum and prejowl regions in all patients seeking facial plastic surgery. 10
As discussed above, the bony mandible below the mental foramen as well as the overlying soft tissues in this region tend to atrophy with age, creating a prejowl sulcus. This sulcus can contribute to the commissure–mandibular groove, also known as the Marionette line, and it can create a jawline irregularity. The commissure–mandibular groove and prejowl sulcus are classic signs of aging. This area frequently benefits from some degree of correction and must be evaluated preoperatively ( Fig. 25.1 ). In the setting of a prejowl sulcus and commissure–mandibular groove, rhytidectomy alone will often not adequately address this irregularity and is significantly enhanced with concurrent mandibular augmentation. 11 Mild prejowl soft tissue deficiencies and commissure–mandibular grooves may often be augmented with filler injections, as well.

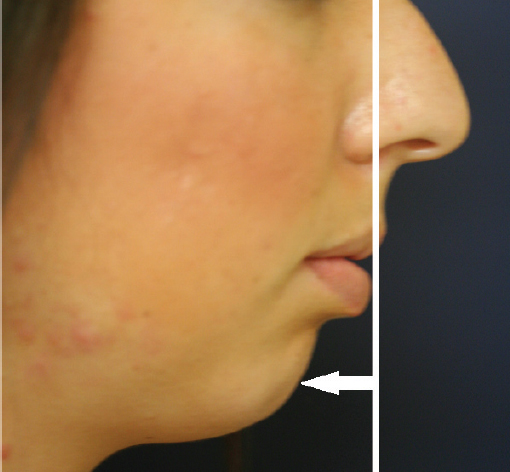
The anteriormost projection of the mandible on lateral view is called the pogonion and should be located at the same projection as the midline vermillion border of the lower lip when the patient is positioned in the Frankfort horizontal plane. While the ideal pogonion for men is at this line, women may tolerate a position 1–2 mm more posterior. 12 When the pogonion is behind this line, the patient has a hypoplastic mentum ( Fig. 25.2 ). Hypoplasia of the mentum may result from micrognathia, which is evident with class II malocclusion, or microgenia, which is the underdevelopment of the mandibular symphysis alone, without malocclusion. Mandibular augmentation is primarily indicated in patients with microgenia or mild micrognathia. In patients with significant micrognathia, however, a discussion about malocclusion and a referral for orthognathic surgery evaluation should take place. Commonly when the mentum is mildly to moderately hypoplastic, the patient will be seen in consultation for another concern, and a hypoplastic mentum may be pointed out as a possible concurrent procedure for an enhanced result.
Importantly, severe microgenia should be viewed as a contraindication to mandibular augmentation until after appropriate orthognathic treatment. Relative contraindications to mandibular augmentation include labial incompetence, lip protrusion, periodontal disease, and shortened mandibular height.
During the initial consultation and throughout the preoperative process, one must closely evaluate for any preexisting asymmetry of the mandible and inform the patient about it, since routine mandibular augmentation will not correct any asymmetry. If a preexisting mandibular disproportion is not discussed until the postoperative period, the patient may blame the resulting asymmetry on the procedure, disrupting the patient–doctor relationship. Custom-designed mandibular–chin implants can be created to improve asymmetry.
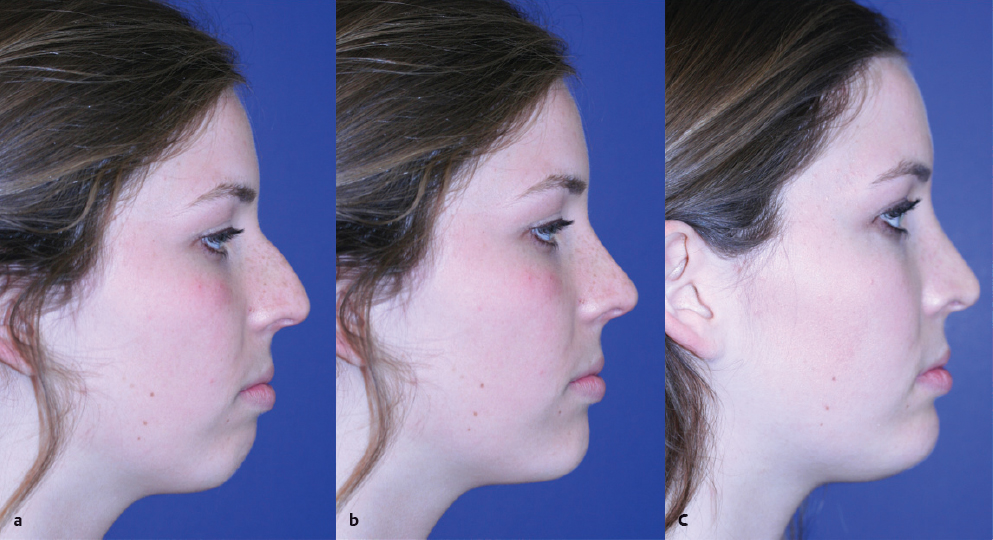
As with any facial plastic surgery procedure, preoperative photography is extremely important. Frontal, lateral, and oblique views should be obtained for surgical planning and implant sizing. Image morphing software can serve as an excellent communication tool between the surgeon and patient with regard to mandibular augmentation. However, preoperative image morphing must be performed with care so that only realistic surgical expectations are conveyed to the patient ( Fig. 25.3 ).
Selecting an Implant
Historically, a number of poorly tolerated materials such as gold, silver, paraffin, and ivory were used for mandibular augmentation and are no longer in use. 13 Currently, in addition to autologous materials, injectable fillers and a number of alloplastic products with significantly improved biocompatibility exist that provide a wide range of options for today’s surgeon. A thorough knowledge of these materials is essential for making the appropriate choice for a given patient. Although briefly overviewed, a detailed discussion of the risks and benefits of all mandibular augmentation options is beyond the scope of this chapter.
Autologous mandibular augmentation with fat, bone, or cartilage grafts can often provide permanent results but requires a second surgical site and may demonstrate variable resorption, possible migration, and uneven contours and bulges that may be difficult to correct. 14 , 15 , 16 , 17 , 18 Injectable fillers, such as hyaluronic acid products (Restylane [Galderma], Perlane [Galderma], and Juvéderm [Allergan]) or calcium hydroxylapatite microspheres (Radiesse [Merz Aesthetics]), are useful for temporary mandibular augmentation, especially at the prejowl groove, and for asymmetries. 19 , 20 , 21 However, subsequent injections are needed to maintain appropriate augmentation and are more costly cumulatively than a single, permanent surgical procedure. Hydroxyapatite cement has also been used for mandibular augmentation. 22 Alloplastic implant materials include solid silicone elastomer rubber (Silastic), expanded polytetrafluoroethylene (Gore-Tex [W. L. Gore & Associates]), high-density porous polyethylene (Medpor [Stryker]), polyester fiber sheeting (Mersilene mesh [Ethicon]), and polymethylmethacrylate (acrylic). The ideal implant material should have the appropriate flexibility and firmness to provide a natural appearance and feel, be nonreactive and resistant to infection, and be readily available in consistent sizes yet easily modified. In addition, it should maintain a stable shape and size over time and, if the need arises, be easy to remove. 23
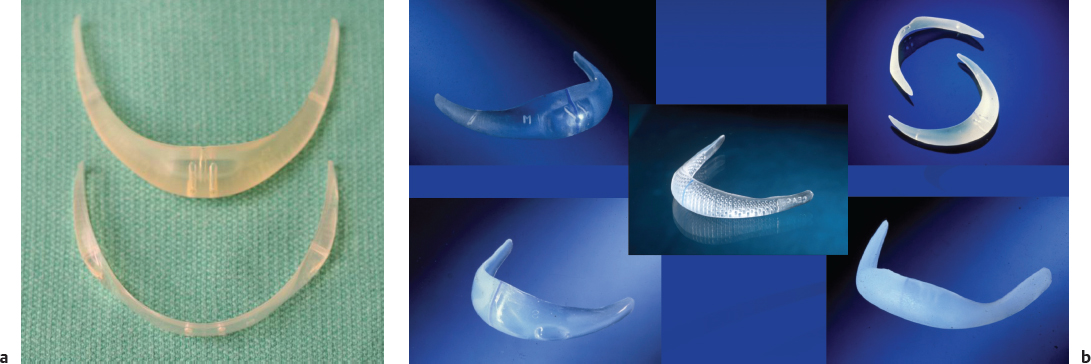
Currently, in the senior author’s opinion, the ideal alloplastic material for mandibular implantation is Silastic. This material is flexible yet firm, can be carved if needed, and, although it does induce the formation of a surrounding capsule, is otherwise nonreactive to surrounding tissue. 23 In the past, central chin implants were commonly used, but they often migrated, resulting in an abnormally pointed appearance ( Fig. 25.4 ). Central implants also did not account for prejowl bony or soft tissue deficiency. Extended mandibular implants, however, have tapered ends that extend to the prejowl region, thereby correcting prejowl deficiency and resulting in a much more natural appearance. The most commonly utilized and researched extended mandibular implants include the extended anatomical chin implant, Mandibular Glove implant (Implantech), Mittelman Prejowl-Chin implant (Implantech), and Mittelman Prejowl Implant (Implantech). Although all of these implants are similar and provide natural results, there are subtle differences between them. The extended anatomical chin implant provides 4 degrees of correction at the mentum but only 1 degree of prejowl augmentation. The Mandibular Glove implant provides some upward vertical tilt of the mentum while extending laterally to the prejowl sulcus, and it comes in five sizes. The Mittelman Prejowl-Chin implant allows for 4 degrees of correction at the mentum as well as at the prejowl sulcus, and it is manufactured with fenestrations for tissue ingrowth and fixation to the mandible. There is also a version of this implant, the prejowl implant, that gives 4 degrees of augmentation at the prejowl sulcus only, without any augmentation at the mentum ( Fig. 25.5 ). Alternatively, there is an additional modification called the Terino Extended chin implant (Implantech) that provides a squared mandibular augmentation that may be appropriate in some male patients. 24 Sizers are available for all of these implants and allow the surgeon to try different implant sizes intraoperatively until satisfied.

Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


