Abstract
This chapter surveys the salient considerations for periorbital rejuvenation procedures. Foremost in the discussion are patient concerns involving function and aesthetics. Areas of emphasis during the presurgical physical examination are listed, and tests for assessing remedial action are thoroughly covered. Common surgical techniques—resection of excess skin, repositioning of anatomical structures, excision of herniated fat pads—are discussed. Measures involved in both brow lifting and upper and lower blepharoplasty are detailed and illustrated, and the chapter concludes with the authors advising on postoperative care, expected outcomes, and complications that can potentially (though rarely) ensue.
21 Browlift and Blepharoplasty
21.1 Goals and Objectives
Understand the proper evaluation of prospective periorbital rejuvenation patients.
Clearly define the benefits for the various periorbital procedures.
Appreciate the technical aspects of addressing each anatomic component of age-related changes and/or neuromuscular abnormalities.
Know the evidence-based perioperative care to maximize patient safety and quality outcomes.
21.2 Patient Presentation
Patients seeking for blepharoplasty or forehead lift present with concerns regarding function, aesthetics, or a combination. Functional impairment may present as a decrease in visual field as a result of senile ptosis, with associated “tired” appearance, or the result of trauma with or without facial nerve paralysis. Other less common neuromuscular disorders such as myasthenia gravis, tumors, or Horner’s syndrome represent a minority of the cases. On the other hand, patients seeking periorbital improvement of age-related changes will be peculiar about what aspect of their appearance bothers them the most. Since the aging face does so at different rate between patients and between anatomic regions in the same patient, a thorough understanding of the patient’s concerns is essential to achieve a satisfactory result. Therefore, the history should include subjective assessment of vision, use of corrective lenses/contacts, symptoms of dry eyes, facial nerve disorders, hypertension, bleeding disorders, endocrine disorders, cataracts, glaucoma, diabetes, corneal or previous lid surgery, psychiatric disorders, trauma, and medications.
The physical examination should document not only any existing skin lesions and dermatologic conditions but also determine the quality of the skin and if chemical or laser peeling would improve the final result. 1 Integrity of the extraocular muscles should also be documented.
A documentation of the orbital fissure will also guide the treatment plan. Guidelines for the aesthetic goals have been suggested by Farkas and Kolar, Flowers, and Wolford et al as follows 2 , 3 , 4 :
The forehead—distance from the anterior hairline to brow—measures 5 to 6 cm.
The distance from brow to orbital rim should be 1 cm; brow to supratarsal crease, 1.6; and brow to midpupil, 2.5 cm. 5
Canthal tilt should be 3 to 4 degrees higher on the lateral canthus. 6 Lid margin to lid fold ranging from 8 to 10 mm. 7
The upper lid may drape over 2 to 3 mm of upper limbus, while the lower lid should just touch the lower limbus. 8
The medial canthus should line up on a vertical plane with the medial brow and lateral edge of the nasal ala. The intercanthal distance should be one-fifth of the facial width. 9 , 10
The upper eyelid exam should evaluate for asymmetries, ptosis, levator function, skin and fat excesses, and lid retraction. The examination must be performed in the resting position and in an elevated brow position if a brow lift is being considered. Further evaluation of the lower eyelid includes assessment of scleral show, lid position, lid tone and support, entropion/ectropion, malar bags, nasojugal folds, and skin/muscle/fat excess. 11
The age-related changes in the orbicularis oculi result in the crow’s feet and contribute to lid ptosis. Such changes are the result of muscle relaxation as well as increasing laxity and attenuation of the orbicularis ligamentous attachments. 12 Observation of the skeletal anatomy is also very important, as a negative vector between the globe, the lower eyelid margin, and the malar eminence also known as “polar bear syndrome” portends an inferior result after lower lid blepharoplasty unless appropriate modifications of lower lid surgery are made. 1 , 8 Finally, documentation of Bell’s phenomenon is important as it is a protective reflex.
21.2.1 Preparation for Surgery
Patient evaluation should begin with a visual field test to assess and validate the need for ptosis correction. Once that is established, bilateral ptosis correction is invariably necessary even if unilateral ptosis is observed. As the pathologic side is corrected, decrease lid elevation reflex will unmask a compensated ptosis on the contralateral side.
Lower eyelid laxity must be assessed with a snap test, and a Schirmer test may be helpful to diagnose dry eyes. Noteworthy is the fact that Rees and LaTrenta found that 65% of patients with postoperative dry eye syndrome had a normal Schirmer test. 13
Next, it is important to determine if brow elevation is indicated. If blepharoplasty is to be performed in combination with brow lift, the eyelids are addressed first to avoid the distortion resulting from edema after the brow lift. It is important to allow for the brow elevation during marking of the upper lids to avoid overcorrection.
Currently, the preferred method of brow lift is the endobrow technique because of comparable brow elevation, long-lasting results, and improved cosmesis. However, if an elevation or advancement of the hairline is intended, then an open technique must be used.
In a healthy patient and with no history of bleeding disorder, no further workup is necessary. Comorbidities are evaluated accordingly.
21.3 Treatment
The goals of periorbital surgery are to restore a youthful appearance. The steps used to accomplish it consist of resection of excess skin, repositioning of the anatomical structures, and excision of herniated fat pads.
The essential elements of a successful operation are judicious resection of redundant skin, fat, and muscle while preserving or restoring symmetry and function. Goals for the upper lid include the restoration of sharp, crisp tarsal folds and a pretarsal show with deepening of the orbitopalpebral sulcus. The lower lids must appear smooth and soft. Distortion of lid shape and position must be avoided. The brow should be elevated to the level of the superior orbital rim in males and 1 cm above in females. It is critical to evaluate both the eyelids and the brow with regard to ptosis.
The procedure may be performed under general anesthesia or local anesthesia plus anxiolytics. If local anesthetic route is chosen, 1 mL of 1% lidocaine with epinephrine is injected on each eyelid prior to the procedure. A diluted lidocaine 0.25% with epinephrine is infiltrated in the forehead and a supratrochlear, supraorbital, and infraorbital nerve block is obtained. With general anesthesia, lidocaine is not necessary and diluted epinephrine 1:1,000,000 is sufficient.
The patient is placed supine with a headband exposing the entire face and ears. Considering the good vascular perfusion and extremely low risk of infection, skin cleansing with peroxide is enough. We believe the peroxide alone is adequate preparation of the skin as long as there is no bone exposure or work performed.
21.4 Brow Lifting
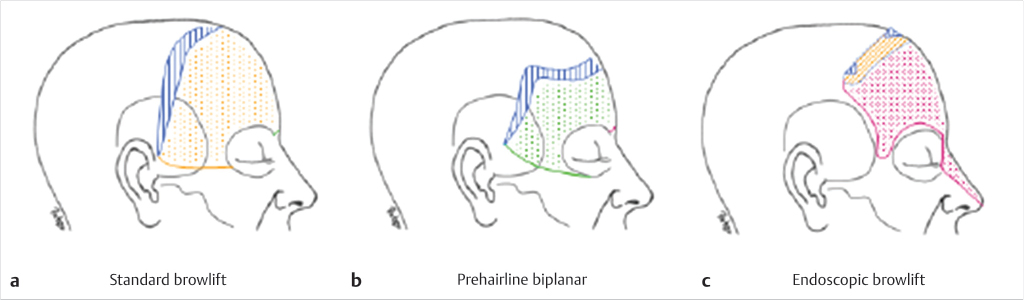
Rejuvenation of the brow is designed to address three main areas: (1) position of the eyebrow, (2) transverse wrinkles, and (3) forehead height (distance from the eyebrow to the hairline). The anatomy of the forehead muscles includes the frontalis which elevates the brow and results in the transverse rhytids. The depressor muscle includes the procerus and corrugators which cause vertical glabellar rhytids and the orbicularis oculi muscle. Various approaches to perform browlift procedures include the standard approach, the pre-hairline incision, endoscopy, direct incision, and upper blepharoplasty approach (Fig. 21‑1).
21.4.1 Open Forehead Lift
Patients with significant to severe forehead ptosis and significant asymmetry of the brows or deep forehead wrinkles may require an open or combined approach. The open approach can be very successful in re-creating lateral brow elevation. The preferred incision varies according to the sex, hair pattern, and desired elevation of the forehead. In females, an incision within the hair-bearing scalp is well tolerated and will hide the scars. It avoids shortening of the forehead, but can result in posterior displacement of the hairline. Therefore, it is best suited for patients with short forehead distances (<6 cm), and should be carefully considered in patients with high hairlines. According to Connell and Marten, every 1 mm of eyebrow elevation produces 1.5 mm of elevation of the hairline. 14 It should also be carefully considered in men at risk for male pattern baldness, as the scar will become apparent with hair loss. In bald patients, superciliary or midforehead incisions can avoid the visibility of a scalp incision and be disguised within the normal transverse forehead rhytids.
Once the incision is made, a subperiosteal dissection will provide the most reliable and lasting elevation. Gentle blunt dissection can be performed with a periosteal elevator. This allows maximum mobilization of the skin and soft tissues. Lateral dissection to release the orbital retaining ligament is helpful in obtaining lateral elevation. Several approaches have been described with particular advantages and disadvantages.
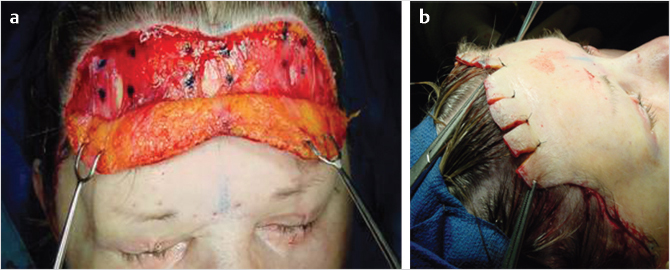
A hairline incision is preferable in patients with long foreheads (>10 cm), as it avoids lengthening the forehead. Incisions are placed perpendicular to the skin and parallel to the hair follicles, as it allows the growth of hair through the scar making it very acceptable to patients. 15 A subcutaneous approach will directly remove the skin attachments to the muscle, effectively addressing the transverse wrinkles (Fig. 21‑2).
21.5 Endoscopic Forehead Lift
Patients with mild to moderate ptosis will benefit the most from this approach. It is also preferable that forehead length is with the normal range of 6 to 10 cm. The principle behind endoscopic forehead lift is that with ablation of the eyebrow depressors, forehead elevation will be unopposed by the frontalis muscle function. Division of the periosteum allows free reposition of the eyebrows and once it adheres to the underlying bone, a natural, dynamic, long-term result can be expected. 16 , 17 Although the use of firm fixation with screws or sutures has been described, physiologic correction alone provides excellent outcomes and helps avoid the undesirable excessively elevated appearance that can occur with rigid suspension of the brow.
Access for the endoscopic cavity is obtained through three triangular incisions marked anterior to the frontal hairline. As indicated, the incisions are beveled to match the direction of the follicles. This helps preserve the hair follicles and avoids alopecia at the scars. The incisions need to be just sufficient for introduction of the endoscopic equipment.
The triangular shape allows for additional access to permit passage of the endoscope through the incision without extending its length. In addition, the horizontal closure of the triangular incision provides a slight amount of extra brow elevation. The three minimal access incisions are placed at the frontal pre-hairline level, one at the midline and the two at lateral incisions in line with the lateral limbus. The size and location can be adjusted to account for asymmetries with regard to forehead ptosis.
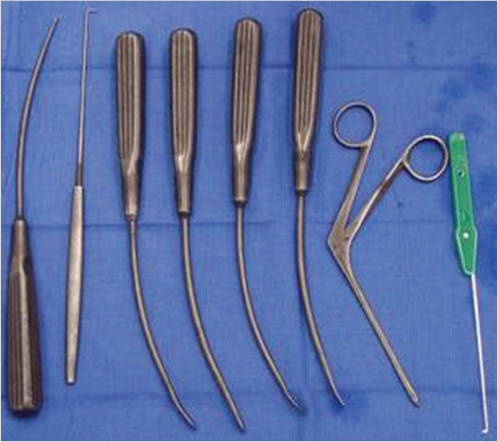
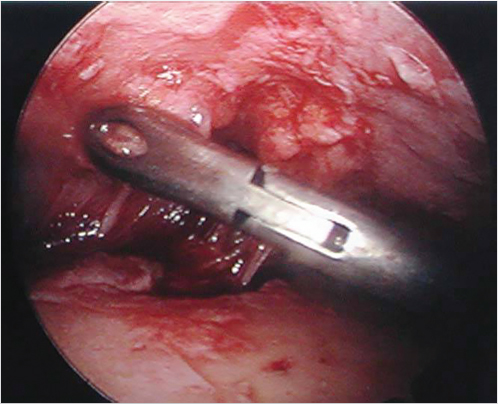
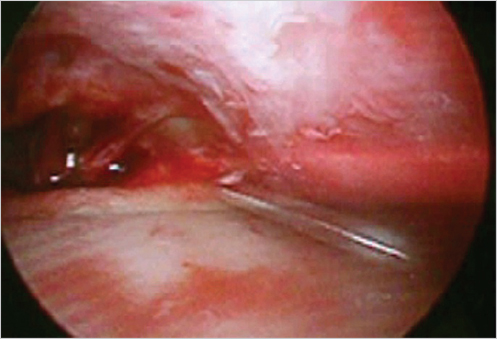
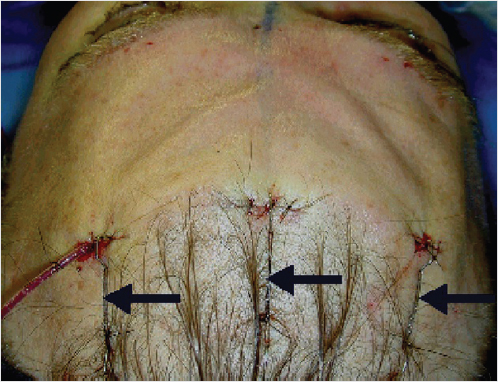
The marked skin and subcutaneous tissue are excised above the musculo-aponeurotic tissue. The galea and the periosteum are bluntly separated with a closed hemostat dissecting along the muscle fibers to avoid damage of the local sensory nerves. Using a curved periosteal elevator, the subperiosteal dissection extends to the supraorbital rims and to the frontotemporal line (Fig. 21‑3). Dissection is extended to the nasal tip to release the procerus. Direct visualization is obtained using a lighted rigid endoscope (Fig. 21‑4) and endoscopic video monitor (Fig. 21‑5). An optical cavity is created using a sheath around the scope to elevate the soft tissue off the lens. In addition, three nylon suspension sutures are placed externally just above the brow line (Fig. 21‑6). Divergent traction is placed on the sutures. The traction on the sutures helps create an optical cavity.



The supraorbital periosteum is divided completely to the level of the lateral orbital rims with an endoscopic carpal tunnel hook knife scalpel. Resection of the corrugators, procerus, and other depressors is achieved bluntly with a grasping forceps. The supratrochlear and supraorbital nerves are identified and preserved. The glabellar region is inspected after resection to ensure that the contour is smooth and not depressed or irregular. If there is any depression, a small amount of fat or SMAS can be used to fill the area (Fig. 21‑7, Fig. 21‑8, Fig. 21‑9).

At the end of the procedure, the incisions are closed transversely. After closure of the access incisions, temporary suspension is obtained with cable sutures. A single staple is placed across the closure of each incision and approximately 4 cm posterior within the hair-bearing scalp. A 3–0 Nylon suture is passed through both staples and tightened to suitably suspend the brow during the immediate postoperative period. This direct, external suspension allows for adjustment to avoid postoperative asymmetries. The staples and nylon sutures are left in place 3 to 5 days. This time period allows for adhesion of the periosteum and long-term effect. The resection of the depressor muscles obviates the need for other methods of suspension. Postoperative suspension has been described with internal sutures securing through tunnels drilled in the external table of the frontal skull or using bone screws. Absorbable tacks are also available to stabilize the soft tissue. A simple method is the use of external nylon sutures thread through staples across the three endoscopic incisions and several centimeters posterior in the hair-bearing scalp (Fig. 21‑10).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


