Abstract
This chapter assists in understanding the anatomy of normal noses and defects requiring reconstruction. A critical issue in nose reconstruction involves aesthetics, and the authors fully address the sensitive considerations of which surgeons should be aware. Treatment options covered include replacement of the bone/cartilage framework, reconstructing the nasal lining, and soft-tissue reconstruction (skin grafts, composite grafts, local flaps, forehead flap). Guidelines involving postoperative care and outcomes conclude the discussion.
18 Nasal Reconstruction
18.1 Goals and Objectives
Understand the typical patient presentation for nasal reconstruction.
Understand the subunit approach to nasal reconstruction.
Clearly define the indications for the various reconstructive options of the nose.
Know the evidence-based perioperative care to maximize patient safety and quality outcomes.
18.2 Patient Presentation
Anatomically, the nose consists of three central elements: external skin, a supporting middle layer of bone and cartilage, and a mucoperichondrium lining. Maintaining the central position of the face, the nose is often considered the most difficult facial feature to reconstruct well. Nasal defects are most commonly encountered after cancer resection or trauma, and reconstruction can vary from simple to complex. Depending on the patient’s age, comorbidities, and aesthetic desire, a less complicated, quicker repair with minimal surgery or stages may suffice. These less complicated reconstructions include healing by secondary intention or suturing the nasal lining and skin together. Both of these techniques will inevitably lead to a permanent nasal deformity or distortion. 1 , 2
The majority of patients want their nasal defect healed without distortion of their appearance. In these cases, the surgeon must be acutely aware of the previous surgical treatments for skin cancer, radiation, trauma, or other scars. These previous interventions may interfere with blood supply, impair healing, or preclude specific flap options. 3 Likewise, operative time, anesthetic requirements, hospitalization, and number of stages must be taken into account prior to choosing a reconstruction option.
18.2.1 Defining the Defect
The defect’s size, depth, site, and surrounding skin condition greatly influence the reconstructive decision. A small, superficial defect is characterized as less than 1.5 cm in size with an uninjured cartilaginous framework. A large, deep defect is defined as greater than 1.5 cm in size and often requires reconstruction of the underlying cartilaginous framework and/or nasal lining. 1 , 2 , 4 However, in all cases, the missing tissue and framework must be replaced in the exact amount. If too little is replaced then this will distort adjacent landmarks and collapse underlying cartilage grafts. Excess replacement tissue will lead to airway obstruction. 1 , 2 , 4 The lateral ala and alar base consist of thick fibrous tissue providing support to alar shape. Full-thickness defects in this area will often need cartilage grafts to prevent tissue contraction, although no cartilage is part of the nascent anatomy.
Topographically, the nose is defined by its nasal subunits, including lateral nasal sidewall (2), alar lobule (2), soft triangle (2), the dorsum, tip, and the columella. 5 These subunits also need to be appreciated in the context of the subunits of the entire face (Fig. 18‑1). Scars that lie within the boundaries of subunits tend to heal in the least conspicuous manner. A superficial defect with a base of healthy, well-vascularized subcutaneous tissue is easily reconstructed with a skin graft. Skin graft reconstruction is best used when the defect is within the nasal dorsum, sidewall, alar rims, or columella, as these areas naturally have thin, adherent skin. 2 Local flaps are a better option when the defect is within the thicker skin of the nasal tip and ala. 6 , 7 , 8 , 9 , 10
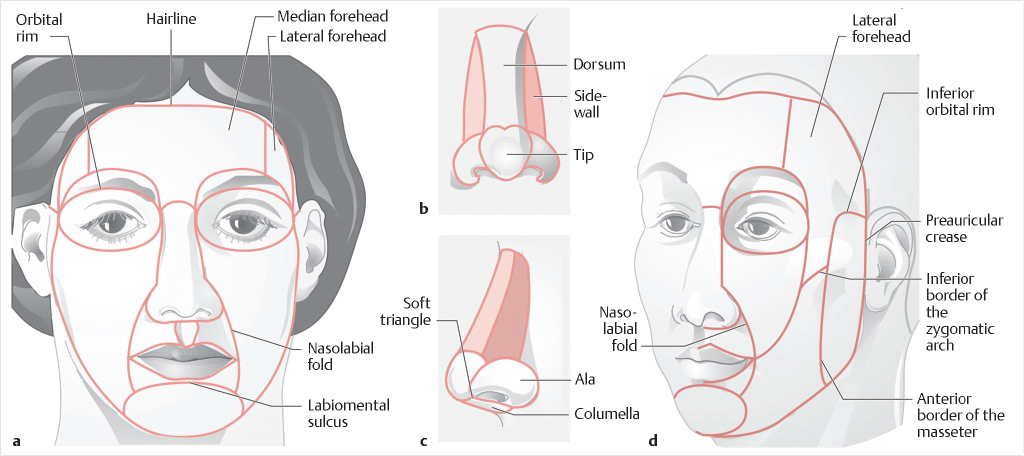
Overall, the process of defining the nasal defect and choosing a reconstructive approach should be thoughtful and comprehensive. The disease process causing the defect, past treatments, patient health, and a review of old photographs should be thoroughly evaluated. The aesthetic subunits need to be appreciated, both for reconstruction of the defect itself and potential use of flaps from the nose or face, in order to provide the best aesthetic outcomes (Fig. 18‑2).
18.3 Preparation for Surgery
For nasal reconstruction, the principles of regional subunit repair are applied. 5 If the defect encompasses greater than 50% of a subunit, then it is recommended that the entire subunit be excised and reconstructed (Fig. 18‑3). It is always the assumption that patients wish to restore their normal facial appearance. Therefore, it is necessary to use the contralateral, normal side of the nose as a guide. In cases of a bilateral nasal defect, use an old photograph. Exact templates are helpful to define replacement tissue dimensions and for marking landmark positions. 2
In instances of severe or complex defects, a preliminary operation is beneficial. The preliminary procedure can help ensure that the margins of the defect are clear of cancer or necrotic debris. It also allows for an intraoperative evaluation under anesthesia and to reopen the airway, if needed. 2 , 4
18.4 Treatment
18.4.1 Bone/Cartilage Foundation
Multiple options exist for the replacement of the bony and cartilaginous nasal framework. The cartilaginous options include septal cartilage, conchal cartilage, and costal cartilage. Bony options include cranial bone and other autogenous bone grafts. 11 , 12 , 13
Septal cartilage provides a strong and straight construct but can be limited in quantity. Conchal cartilage is often useful for alar batten grafts and tip shaping, including replacement of lower lateral cartilage (Fig. 18‑4). It is weaker than septal cartilage and has an intrinsic curve. Costal cartilage is taken from the sixth through ninth ribs and provides a strong construct. However, this cartilaginous option does produce donor-site morbidity and has a tendency toward warping over time.

For nasal reconstruction requiring bone grafts, cranial bone can be harvested from the parietal area. These bone grafts are useful in reconstructing the bony nasal pyramid, but are prone to resorption and distortion. Other areas for bone graft harvest are the ribs and iliac crest. Likewise, these are subject to resorption and donor-site morbidity.
18.4.2 Nasal Lining
When reconstructing the nasal lining, there are several considerations. The first is to use a well-vascularized flap to provide internal support for needed cartilage or bone grafts. The second is to select a material thin enough to prevent airway obstruction. The flap must also not distort the structural framework of the nose by tension or contracture. Several options are available. 11 , 12 , 13
The nasal turnover flap has limited vascularity and is thick. The nasolabial flap, although with good vascularity, is bulky and may require multiple stages. The forehead turn-in flap has good vascularity but is also bulky and may require multiple stages. A septal mucoperichondrial flap is well vascularized and useful in reconstructing the nasal midvault and alar domes. This flap is a large, caudally based rectangle of mucosa or mucosa and perichondrium. A mucosal advancement flap is a bipedicled flap with limited availability but highly vascularized. This flap option is capable of supporting primary cartilage grafts. A septal door flap involves folding down the ipsilateral nasal mucosa and then “swinging” a septal door of contralateral mucosa with septal cartilage. Care must be taken to leave a sufficient amount of septum to prevent instability. The facial artery musculomucosal (FAMM) flap is superiorly based on the facial artery axial blood supply. To reconstruct nasal lining by free tissue transfer, the radial forearm is the most commonly used donor site. This method of nasal lining reconstruction is performed in multiple stages and requires aggressive thinning. To reduce the number of stages required, prelaminated flaps can be created. For prelaminated flaps, skin grafts or mucosal grafts can be placed on the undersurface of free flaps or forehead flaps to create the nasal lining prior to transfer. Cartilage grafts can be placed between the healed, vascularized, laminated layers of the transferred flap.
18.4.3 Soft-Tissue Reconstruction
Skin Grafting
Skin grafting to reconstruct a nasal defect is advantageous in that no new scars are added to the nasal surface. The locally available excess tissue does not limit this technique. Historically, skin grafts for nasal reconstruction are harvested from preauricular, postauricular, supraclavicular, or forehead donor sites. 1 , 2 The quality of the donor skin graft is compromised by the transient ischemia incurred prior to imbibition and inosculation. This transient ischemia leads to a pale, smooth, and atrophic appearance of healed skin grafts. The preauricular skin provides a better skin color match when healed, especially when correcting a defect within the nasal sidewall or columella. Postauricular skin grafts remain red in appearance. Supraclavicular skin grafts heal with a brown and shiny appearance. The forehead skin and underlying fibrofatty subcutaneous layer make this donor site thicker, stiffer, and more ideal for resurfacing nasal defects of the tip and ala.
First, a pattern of the nasal defect must be created prior to debridement to ensure a clean and vascular wound bed. If a pre- or postauricular skin graft is chosen, elevate the graft within the subcutaneous layer. A forehead skin graft should be elevated superficial to the frontalis muscle. With curved iris scissors, the skin graft is thinned to the thickness of the nasal defect. Next, the skin graft is transferred onto the prepared recipient site and inset using a single layer of sutures placed around the periphery. A bolster is then affixed on top of the skin graft with tie-over sutures to prohibit lateral shearing or fluid accumulation underneath the graft. The bolster is best left in place for 7 days. Initially, the skin graft will appear white in color, and then gradually change from blue to pink.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


