20 Neuromodulators
Key Concepts
A thorough history and physical exam allow for appropriate selection of patients who will benefit from injection while avoiding those who will likely not respond well to treatment or be placed at greater risk.
A comprehensive understanding of the relevant anatomy of the upper face and muscular interactions is imperative for proper injection technique and optimal outcomes.
Injection over the glabella and at the level of the brow, while avoiding injection 1 to 2 cm above the brow, will provide optimal results and prevent medial brow ptosis, a common adverse effect.
Small amounts of neuromodulator can be injected into the frontalis muscle to help smooth the forehead without risk of significant depression of the brow.
Introduction
Since its initial application in the treatment of strabismus in children in the 1970s and 1980s, botulinum toxin type A′s usage has grown exponentially.1 Botox (Allergan, Irvine, CA) has become a layperson′s term, and the procedure, once reserved to subspecialized corners of medicine, today is performed by practitioners from many branches of medicine, for applications cosmetic and functional. Botulinum toxin′s U.S. Food and Drug Administration (FDA) indications currently include blepharospasm, strabismus, and dynamic glabellar rhytids.2 However, its multiple off-label uses include lateral orbital rhytids, dynamic forehead lines, peau d′orange of the chin, platysmal bands, hyperhidrosis, and migraine headaches, to name a few.3
Three botulinum neuromodulators are currently available, having obtained FDA approval for cosmetic use in July 2011: onabotulinumtoxinA (Botox Cosmetic, Allergan), abobotulinumtoxinA (Dysport, Medicis Aesthetics, Scottsdale, AZ), and incobotulinumtoxinA (Xeomin, Merz Pharmaceuticals, Frankfurt, Germany). Myobloc, a botulinum toxin type B, demonstrated encouraging results in the treatment of hyperfunctional frown lines but fell out of favor largely because of its short duration of action and the pain associated with its injection.4,5
Because of their ease of use, quick results, and long history of safety, botulinum neuromodulators have become nearly ubiquitous in aesthetic medicine. However, the astute clinician must possess a sound knowledge of neuromodulator physiology, relevant anatomy, and potential complications to successfully treat patients.
Background: Basic Science of Procedure
Botulinum neuromodulator exists as a two-chain polypeptide consisting of a 100 kD heavy chain and a 49 kD light chain joined by a disulfide bridge. The light chain functions as a protease, cleaving a critical protein in the fusion of acetylcholine vesicles in the presynaptic nerve terminal at the neuromuscular junction. Synaptosomal-associated protein 25 (SNAP-25) is the protein cleaved by the type A neuromodulator, whereas vesicle-associated membrane protein (VAMP), syntaxin, and synaptobrevin are proteins cleaved by other neuromodulator serotypes (B through G). By preventing fusion of the acetylcholine vesicle with the presynaptic axon terminal membrane, acetylcholine is not released into the neuromuscular cleft. This causes the target muscle to be weakened reversibly until new presynaptic vesicles can be generated. This regeneration period varies, based on the target muscle, dosage, and neuromodulator, but it is thought to be 3 months.6
Botulinum neuromodulator is rapidly denatured at temperatures exceeding 60°C. Therefore, both onabotulinumtoxinA and abobotulinumtoxinA are to be stored at temperatures between 2 and 8°C, before and after reconstitution. One purported advantage of incobotulinumtoxinA is its lack of need for refrigeration in transport and prior to reconstitution. This occurs because incobotulinumtoxinA is manufactured as a 150 kD protein without the accessory proteins found in nature and other formulations. The accessory proteins serve to stabilize botulinum toxin but must be kept at low temperature to prevent denaturation. Without accessory proteins, incobotulinumtoxinA continues to demonstrate long-term stability and potency, thus allowing for unrefrigerated transport of vials.7
Pertinent Anatomy
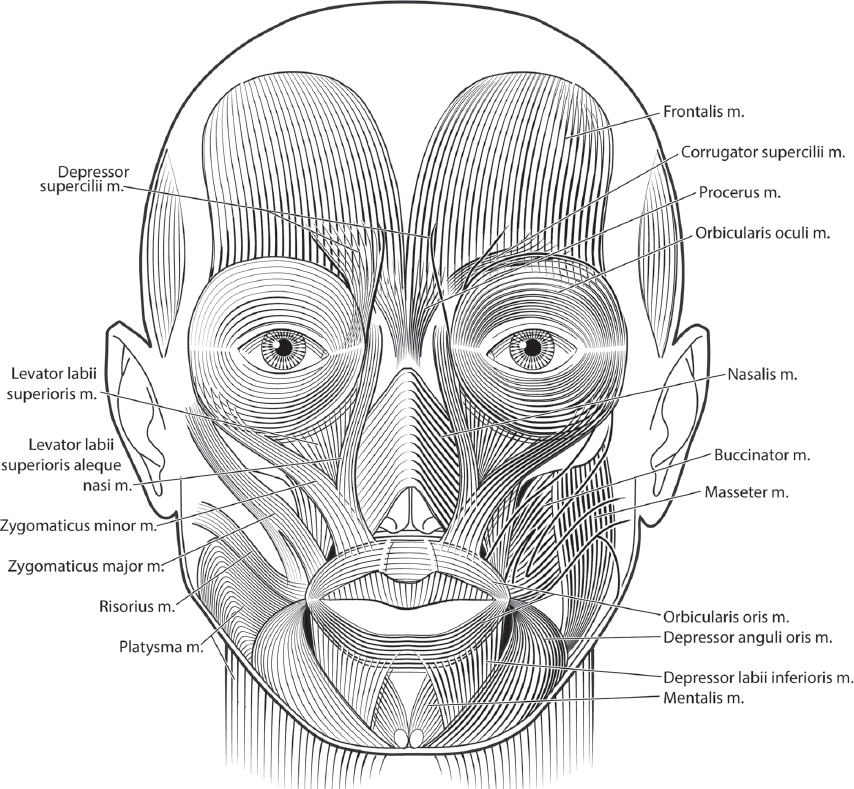
The injecting clinician must possess a sound knowledge of facial anatomy before embarking on any treatment, surgical or otherwise. Because neuromodulators target facial muscles, particular attention must be paid to facial muscular anatomy. It should be noted that anatomy can vary slightly between patients, genders, and races, but over all, it is fairly consistent ( Fig. 20.1 ).
Brow
The paired corrugator supercilii and procerus muscles constitute brow musculature. However, the inferior frontalis and superior orbicularis oculi are also in the region and must be recognized with any brow intervention.
The procerus originates from the nasal bones and inserts into the subcutaneous tissues between the medial eyebrows as a flat, unpaired muscle in a vertical orientation. Procerus contraction produces characteristic transverse nasal lines at the nasion.
The corrugator supercilii is a thick, paired muscle originating at the procerus medially and inserting laterally into the orbicularis oculi at the lateral brow. Corrugator contraction produces glabellar frown lines in a vertical orientation medial to the medial clubhead of the eyebrow. Many textbooks erroneously depict the corrugator as a long, vertically oriented muscle extending well into the midforehead. While there is a small subset of patients in whom the muscle takes an oblique course instead of paralleling the eyebrow, they exhibit more of an oblique rhytid and not the classic vertical line.
Forehead
The frontalis muscle is responsible for horizontal forehead lines, which trouble many patients. It originates in continuity from the galea aponeurotica superiorly and interdigitates with the procerus, corrugator supercilii, and orbicularis oculi muscle inferiorly. Most often, the muscle displays a midline dehiscence, creating two distinct bellies, rather than a single flat muscular sheet. Contraction of the frontalis causes elevation of the brow but also results in dynamic horizontal lines, which become curvilinear laterally.
Periocular Area
The orbicularis oculi encircles each eye as a wide, flat muscle. It extends out from the upper and lower eyelids and on to the brow and cheek. Medially, the muscle inserts into and around the medial canthal tendon and lacrimal sac, enabling a pumping action of the sac contents into the nasolacrimal ductal system. Laterally, a ligamentous contribution from the orbicularis oculi is dealt to the lateral canthal tendon, though this contribution is quite minor.
Contraction of the orbicularis oculi causes a sphincteric closure of the eyelids over the globe. As a result, lines tangent to the muscle project radially. In the lateral orbital area, these radial lines are better known as lateral orbital rhytids or crow′s feet. It should be noted that in addition to its eye closure function, the orbicularis oculi is also the most powerful depressor of the brow.
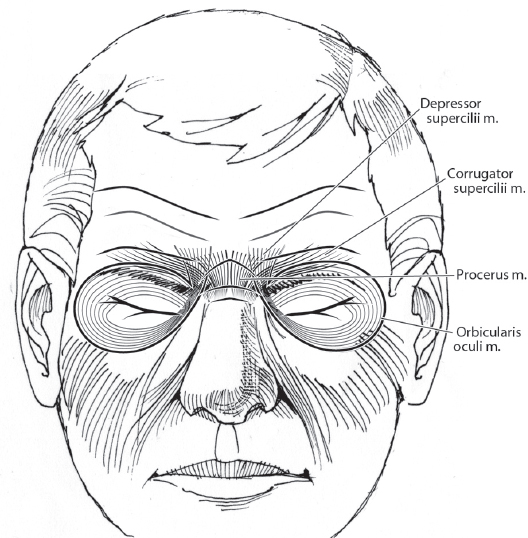
Lower eyelid lines result from photoaging of eyelid skin. These lines may be accentuated by the underlying orbicularis oculi muscle. However, because the primary function of the orbicularis oculi in this area is closure of the lower eyelid, a fine balance exists between smoothing fine lines and causing ectropion. The muscles involved in facial expression are seen in relation to the overlying skin in Fig. 20.2 .
Nose
Although nasal appearance is largely determined by bony and cartilaginous architecture, muscular anatomy can cause subtle aesthetic problems. A principal muscle on the nasal midvault is the paired, fan-shaped nasalis. Originating at the inferior nasal pyriform aperture, it travels transversely to insert into the aponeurosis of the contralateral muscle.3
Contraction results in “bunny lines.” The depressor septi is an unpaired muscle at the base of the nose innervated by the buccal branch of the facial nerve. Arising from the incisive fossa of the maxilla, it inserts into the caudal septum. Its function is to constrict the nares. However, in doing this, the muscle also brings the nasal tip inferiorly (droopy nasal tip), particularly with a smile. As such, it has been postulated that its transection during rhinoplasty can help to alleviate the “smiling deformity.”8
Perioral
Similar to the orbicularis oculi, the orbicularis oris functions as a sphincteric muscle encircling the mouth. Contraction of this muscle closes, protrudes, and purses the lips. The upper lip segment inserts into the maxilla just superior to the canine, and the lower lip segment originates on the mandible just lateral to the mentalis. Laterally, the orbicularis oris interdigitates with the depressor anguli oris (DAO) inferiorly and the risorius at the oral commissure.9 Because of its sphincteric function, radial lip lines can result, often called smokers’ lines, though most patients exhibiting them do not have a history of smoking. These lines can become particularly apparent in females as lipstick can bleed into the depths of the lip lines.
The DAO originates at the oblique line of the mandible and inserts at the modiolus of each oral commissure. The DAO′s contraction pulls the oral commissures inferiorly and can cause a chronic downturned commissure resulting in a frowning appearance. Its opposing muscles are the risorius and zygomaticus major, which serve to elevate the oral commissure.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


