2 Breast Aesthetics
Summary
This chapter serves to provide an insight into the aesthetics of the female breast, a woman’s appreciation of her anatomy and the important aspects of assessment of breast aesthetics in achieving satisfactory aesthetic or reconstructed outcome from any given procedure.
Key Teaching Points
A surgeon should have a full appreciation of normal breast aesthetics.
An attempt should be made to understand the goals of the patient in achieving a pleasing outcome, particularly when her desires may differ from those of her surgeon.
The normal 45:55 balance of the best profile should be aimed for as an aesthetic goal.
Cleavage formation is partially dependent on the position of the origin of the pectoral muscle as well as that of the breast.
Different areas of the breast skin envelope scar differently.
Anatomical boundary should be respected.
2.1 Introduction
Breast surgery is an artistic endeavor, an exercise in right-brain creativity. Clarification of patient expectations and knowledge of individual anatomical characteristics are critical to the surgical plan, but ultimately it is an internalized vision of what is normal and aesthetically pleasing that guides the procedure.
Clinical Pearl
In planning breast surgery, it is important to first visualize the most attractive breasts for the patient and then work backward, selecting reliable techniques that will help attain a result that will meet her expectations and mine.
Clinical Pearl
I know of no shortcuts to teach this aesthetic judgment. It exists in different degrees in each of us and is manifest in the creativity, skill, and artistry of the surgical results we produce.
Techniques and technological innovations are not the answers but rather the tools to be guided by personal artistic vision and careful preoperative assessment.
Achieving an “ideal” aesthetic outcome in breast surgery is a desirable but elusive goal. Although standards of beauty exist and define the ideal breast, these standards cannot always be approximated through surgery. Sculptors may reshape their clay with abandon until they achieve the desired effect; surgical artists, however, are limited in their search for the perfect, the normal, the well-formed breast by the nature, limitations, and viability of the materials they mold.
To be successful, the surgical plan must anticipate the expected alterations in breast appearance, form, and shape that invariably result from wound healing, maturation, and settling of the tissues after the operation.
It must also accommodate changes associated with placement of foreign bodies or movement of autologous tissues.
Surgeons’ tools are tissue, muscle, and skin, and every incision or transfer of tissue results in scars and changes that cannot be erased. Furthermore, each patient heals in a unique manner. Surgeons must understand how each procedure affects healing and the result as it “ages.” After breast implant surgery, the tissue ages differently than after breast reduction operations, which in turn mature differently than after autologous flap procedures. Unilateral procedures, particularly with implants, also produce longitudinal aging disparities.
The surgeon’s primary goal is to understand the patient’s aesthetic ideal and to plan a procedure that will meet the patient’s expectations as closely as possible; her psychological well-being is closely tied to the success of the operation and the excellence of the result. To create breasts that approximate this aesthetic norm while satisfying the patient’s aesthetic expectations, the surgeon must develop a concept of the normal, attractive breast, with knowledge of the anatomical landmarks and proportions that contribute to it. Only then can a surgical approach be planned for the individual patient with an idealized goal in mind.
Breast aesthetics are based on two senses: the visual and the tactile. A woman’s breasts must not only look good, they must also be sensitive and feel normal. Softness, warmth, smoothness, mobility on the chest wall, and sensitivity to touch, particularly in the central breast and nipple–areolar region, are all important aspects of the normal breast. Observable visual aesthetic characteristics of symmetry, flow, contour, and proportion combine with the sensual to produce attractive breasts.
2.2 Shape
Breast development is usually complete when a young woman attains her final height, somewhere between 13 and 16 years of age. Normal aesthetic development leads to fully rounded, hemispherical, symmetrical pubertal breasts. At that time, reflecting the influences of individual genetic, hormonal, gravitational, and postural changes, the upper portion of the breast usually becomes less convex, appearing flattened as the breast parenchyma settles, and the lower portion of the breast becomes fuller. The breasts gradually assume a more mature look by settling downward and laterally, with relatively more tissue retained in the lower pole of the mature breast. This general direction of change in form continues with the aging process as the breasts develop additional glandular ptosis that is reflected in a general settling of the breast and an upper pole breast flattening, with stretching and descent of the gland and nipple–areola.
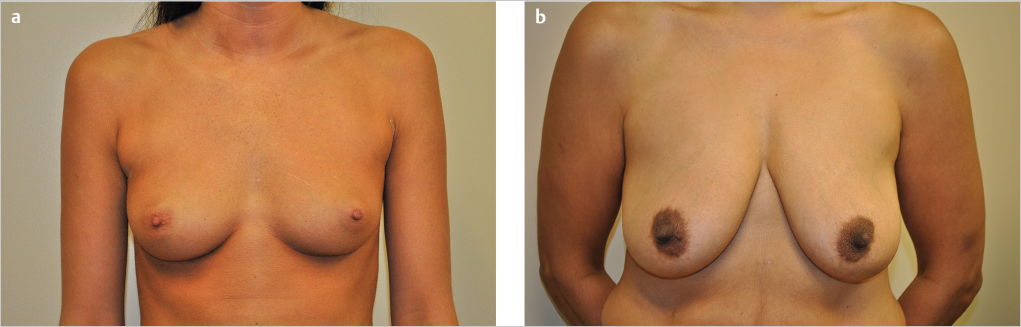
After the breasts have fully developed, their shape is influenced by the quality and elasticity of breast skin, the volume and position of breast parenchyma, the changes associated with aging, and the quality of musculofascial support. A number of life factors contribute to variations in what we consider “normal” breast shape. For example, women with thin, inelastic skin or women who have lost breast parenchyma volume are prone to striae and may lose breast skin support, thereby developing early ptosis, especially if the musculofascial attachments (Cooper’s ligaments) also become attenuated and inelastic (▶Fig. 2.1).
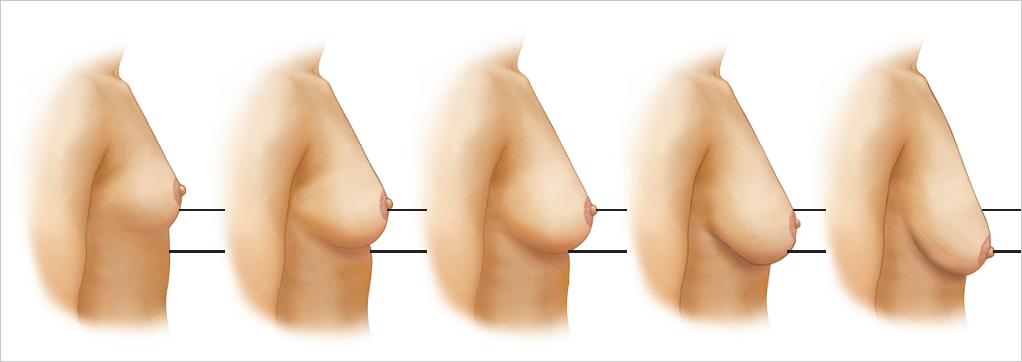
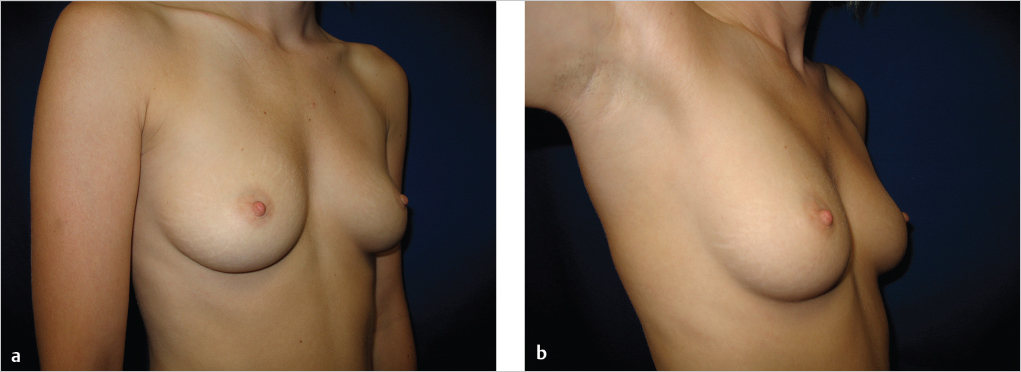
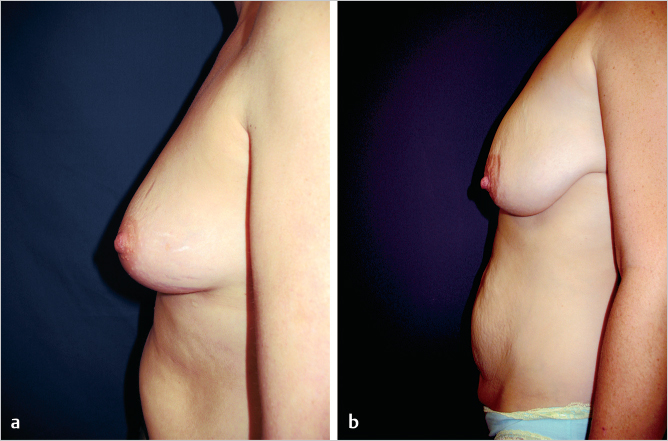
Cyclic breast volume changes may produce stretching, which can lead to a premature aged appearance. Pregnancy and lactation expand both the parenchyma and the overlying breast skin and stress the musculofascial ligaments. The skin’s expandability, resiliency, and elasticity may also be affected by varying degrees of tightening when these cycles are completed and by the effects of high hormonal levels that weaken the fascial support and allow it to stretch. Fluctuations in weight (affecting body and breast parenchyma fat content) also change breast volume as well as the ratio of volume to skin and deeper fascial support and can therefore lead to changes in the normal “ideal” breast shape (▶Fig. 2.2). As breast size increases, the nipple–areolar position progressively moves inferiorly and laterally.

2.3 Aesthetic Considerations
2.3.1 Breast Shape
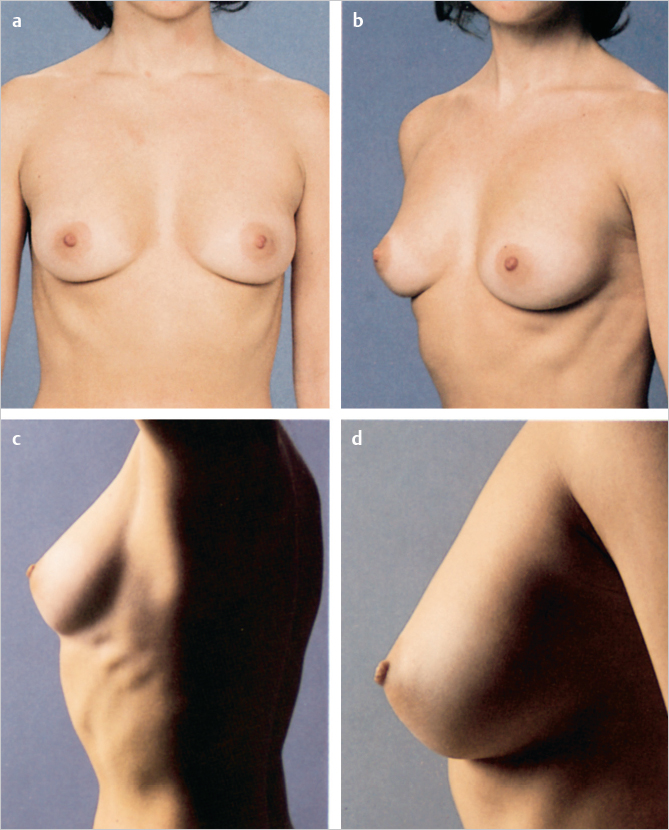
A breast surgeon needs to have an ideal model to work from in analyzing each patient, fully recognizing normal breast variations. This ideal breast shape exhibits elastic skin cover and support, strong, deep fascial attachments, and a breast volume in the range of normal, generally between 300 and 500 g. An understanding of ideal breast proportions is also essential. On frontal view, the breast is less full above the areola in the upper pole and fuller below, especially lateral to the areola in the lower pole. The breast is located over the anterior lateral chest with a lateral inclination of 45 degrees. Breast volume and contour are in harmony with the proportions of the chest, torso, and buttocks. Laterally, ideal breast appearance would again reflect good cutaneous and fascial support, with the breast parenchyma positioned above the inframammary crease, a subtle fullness above the areola, and a roundness and convexity below (▶Fig. 2.3).
2.3.2 Nipple–Areola Position and Appearance
Lines of contour all flow to the nipple–areola, the focal point of the breast. Nipple–areolar position, size, color, texture, inclination, and symmetry are related to and define breast form and function. Reference points for determining nipple–areolar location extend from the sternal notch and midline to the umbilicus, the midclavicular point, and the midbreast line, and from the midbreast line to the midclavicular point to the anterior superior iliac spine.
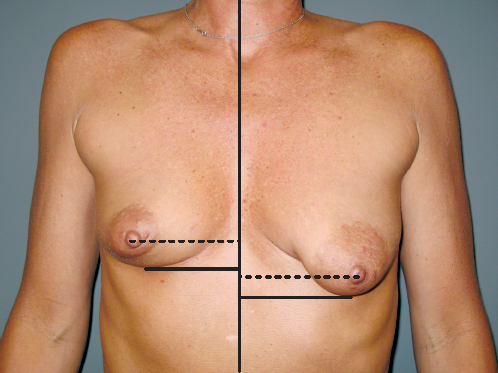
The nipple is situated on the midbreast line approximately 19 to 21 cm from the midpoint of the clavicle. This breast line begins at the midclavicular point and continues through the nipple to the inframammary crease. A horizontal line at the level of the nipple further defines the upper and lower breast quadrants. Malucci studied what were considered ideally shaped natural breasts and determined that in the upright position, approximately 55% of the breast volume is below this transverse line and 45% above it (▶Fig. 2.4).
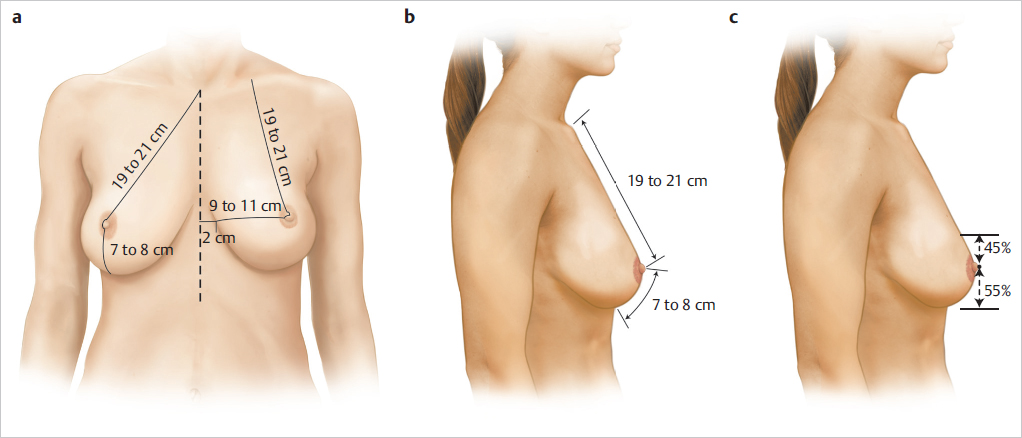
The nipple has a normal 10 to 15% medial and slight upward inclination, and it is usually situated 9 to 11 cm from the midsternal line and approximately 13 cm from the midaxillary line, typically the lateral extent of the breast.
The distance from the nipple to the inframammary fold is 7 to 8 cm, depending on breast size, volume, maturation, and degree of ptosis. The vertical measurement over the breast from the clavicle to the inframammary crease is 26 to 29 cm; the lateral width is approximately 18 to 22 cm from midline to lateral breast line; and the breast base, providing coverage of the underlying musculofascial layer, is 11 to 14 cm. An areolar diameter of 35 to 45 mm is usually judged attractive, as is a nipple diameter of 5 to 8 mm and a nipple projection of approximately 4 to 6 mm (▶Fig. 2.5).

The areola projects from the breast mound. The areolar diameter in relation to the overall breast size varies; it can become stretched disproportionately from mammary hypertrophy. Areolar diameter is a consideration in planning a reduction mammaplasty; many patients have a preference in areolar diameter, and this should be elicited during preoperative planning. With a tight skin envelope and a medially and laterally constricted breast associated with less support centrally because of the thin dermis of the areola, central protrusion of breast parenchyma can produce a tubular breast deformity. The nipple protrudes centrally from the areola; its projection increases when it is erect. Large areolae containing a significant portion of breast parenchyma are commonly seen in patients with tubular breasts (▶Fig. 2.6).
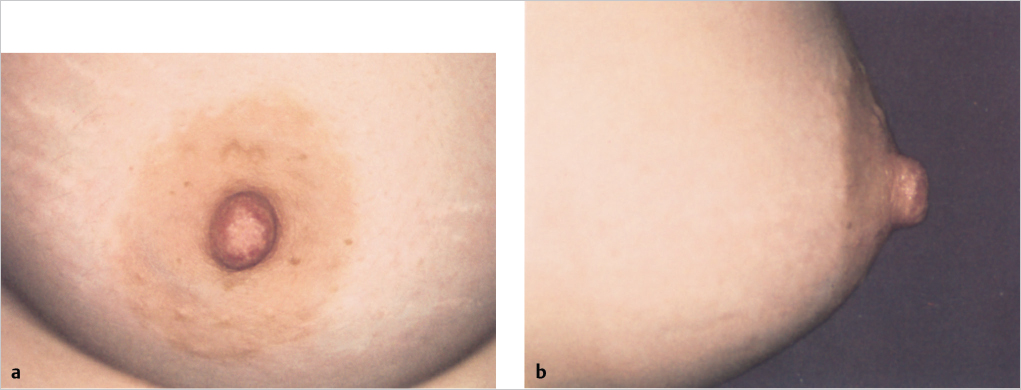
The areola has distinct coloration and skin textures that are subject to hormonal and genetic influences as well as the natural changes associated with aging. Characteristically the areolar pigmentation is darker than that of the surrounding skin. Nulliparous women have a light brown or even pinkish areola. The color usually darkens with hormonal and solar exposure as well as during pregnancy and after delivery, and then usually lightens several months after lactation, but not to its original shade. It has a firm texture with a corrugated surface produced by the muscles and Montgomery’s glands within. Areolar pigmentation often decreases after menopause and the natural decrease of estrogen and progesterone. The nipple is frequently more deeply pigmented than the areola (▶Fig. 2.7).
2.3.3 Breast Flow
The breasts are an aesthetic mixture of soft curves and flowing lines. Situated on the chest wall in an anterolateral position, the breasts flow gently from the clavicles onto the chest wall, over the upper abdomen, and from the axilla—key anatomical juncture points. From above, the breasts flow from the clavicle and contribute fullness along with that supplied by the axillary fold, which consists of the pectoralis major muscle and tendon, axillary breast tissue, and subcutaneous tissue. Flow continues from the clavicle downward to the breasts and projects forward to the nipple–areolae, which are inclined slightly upward and outward. As breast size increases, this nipple–areolar position progressively moves inferiorly and laterally.
Below the areola, breast fullness and convexity increase, and the breast curves downward to a slightly concave inframammary juncture with the upper abdomen at the inframammary line or fold. This breast–abdomen juncture, the inframammary crease, begins medially near the sternal midline and curves gently downward to the midbreast line; it then curves upward slightly and diffuses near the anterior axillary line at the lateral breast border and the lateral chest and may be continuous with the lateral breast line. A more lateral takeoff of the inframammary crease is a forme fruste of constricted breasts. The ideal breast profile has a smooth breast projection in balance with posterior buttock projection. The breast profile from the clavicle to the second and third ribs is practically vertical, with a subtle suggestion of fullness. In thinner women, there is a distinct lateral breast crease near the anterior axillary line, which is lost when increased body fat fills this area and creates lateral chest fullness.
Breast projection begins at the level of the second and third ribs, flowing downward and outward to the nipple, located at the level of the fourth and fifth rib interspaces. The areola projects slightly from the surrounding breast tissue and the nipple projects centrally and more prominently. The nipple is above the level of the inframammary crease, which is usually located at the sixth and seventh rib interspace; breast flow downward to this crease is slightly convex. Over time, age, gravity, breast volume, and decreased elasticity contribute to a gradual lowering of the breast landmarks relative to the underlying musculoskeletal system as a woman gets older and experiences normal physiologic changes. The extent of this descent depends primarily on the volume of the breast and the elasticity of the tissues (▶Fig. 2.8).
2.4 Cleavage
The development of cleavage depends on both the medial origin of the pectoralis major muscle and the medial most extent of the breast parenchyma. Cleavage is not necessarily a function of large breast volume. Women with a deep, natural cleavage tend to have a very medial sternal breast boundary, whereas women with no cleavage often have a medial breast border that commences laterally over the costal cartilages rather than parasternally. As the breasts enlarge, fullness usually develops inferiorly and laterally. With increased volume, the influence of gravity, and the development of ptosis, the breasts appear to diverge and fall away from the midline laterally and inferiorly. When a woman is supine, the breasts flow laterally, sometimes even beyond the actual chest wall.
Cleavage is an aesthetic goal for many women seeking breast surgery; they desire the appearance of a full cleavage that will be evident in low-cut clothing or bathing suits. It is important to emphasize to these patients that unless natural cleavage exists de novo, it is unlikely that it will be created with the insertion of an implant, however, medially it is placed. Most photographs of women with full cleavage are taken while their breasts are artificially pushed upward and medially with brassieres or other supports. Women who desirea full cleavage without bra support are often disappointed with aesthetic and reconstructive breast operations unless it is pointed out that this cleavage isthe product of substantial support combined with medial breast flow. Breast implants may be used to provide upper breast fullness; however, these do not always create a natural-appearing solution, particularly in cases in which the normal breasts flow over these devices (▶Fig. 2.9).
2.4.1 Symmetry
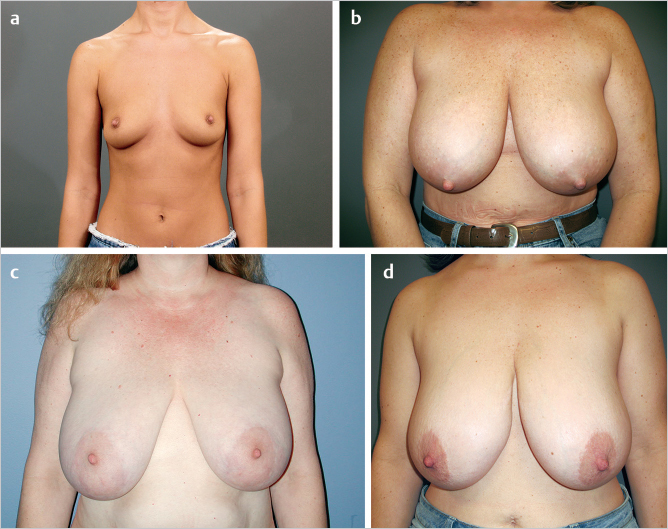
Symmetry is key to aesthetic breast appearance. Ideally, breasts should be comparable in size, shape, and degree of ptosis. Most individuals feel that their bodies are not “right” unless they are balanced and symmetrical (▶Fig. 2.10).
Perfect symmetry, however, rarely if ever exists in nature and is even more of a rarity after breast surgery. It is normal for some asymmetry to be evident in paired body structures, and the breasts are most likely to be naturally asymmetrical. In fact, it is the unusual woman who does not demonstrate some breast, nipple–areolar, or chest wall asymmetry. For example, one side of the trunk is usually larger than the other. Additional disparities may be seen in muscle development or in the underlying skeleton in the costal region, particularly when there is scoliosis or other curvature of the spine.
These natural asymmetries should be pointed out to the patient, discussed, documented during the preoperative evaluation, and included in the development of the treatment plan. Even when a woman’s breasts appear symmetrical, at some point healing and aging will accentuate any minor asymmetries that are present.
2.4.2 Ptosis
Some breast ptosis is a normal, desirable component of the mature breast, since it contributes to natural contour, mobility, and definition. The nipple position relative to the breast parenchyma also affects the aesthetics of breast ptosis. Ptosis becomes undesirable when the nipple points downward and the breast parenchyma predominates below the areola and droops on lateral view considerably beneath the inframammary crease. This degree of ptosis gives the breasts an aged appearance. Most women accept the increased lower breast fullness but object to the upper breast flatness and desire a visible nipple position. Providing additional upper fill with breast implants or with a pedicle flap of lower breast parenchyma is a consideration for these patients (▶Fig. 2.11).
2.5 Clinical Application of Breast Aesthetics
Surgical modifications and postoperative breast appearance are evaluated based on the surgeon’s and patient’s aesthetic standards. Are the breasts symmetrical? Are the size and proportions correct? Are the breasts softly contoured, with appropriate flow and definition? Are the incisions and scars hidden? Is breast appearance natural? Is the patient satisfied? Are her expectations met?
Clinical Pearl
There is nothing more frustrating than a result hailed by the surgeon as an aesthetic triumph that the patient views as a failure. It is imperative for the surgeon to understand the patient’s expectations and to attempt to incorporate them as much as possible into the operative plan.
What happens when the general body proportions are not ideal, when the surgeon is faced with a patient who is shorter, heavier, or thinner than the mean? How does one modify the approach, adapt aesthetic standards to individual patients, and produce attractive, symmetrical breasts that are proportional to the patient’s body type and compatible with her aesthetic ideals?
2.5.1 Adjustments for Different Body Types
Breast shape and size should be proportional to individual body type; body proportions and body fat content will vary, and those variations require alterations in the surgical planning process. To explore the possibilities for surgical modification, let us consider five different body types.
Slender, Angular Bodies
Tall, thin women with a low percentage of body fat present a surgical challenge. Frequently any asymmetries are accentuated by smaller breasts that lack the layer of subcutaneous fat necessary to “soften” underlying irregularities. Usually structures of the breast and adjacent areas are more sharply defined in these slender patients and even the slightest breast irregularity or change in symmetry or appearance is more noticeable. The thin skin is often elastic and not attenuated by underlying volumetric expansion. Such skin tends to retract when incised, is difficult to expand, and may heal with widened scars, with the younger, thicker dermis stimulating wound healing with scar proliferation and hypertrophy. Accordingly, procedures using hidden or minimal scars are preferred. These patients often lack lower breast overhang at the inframammary crease and have minimal breast projection; therefore, there is little potential for hiding scars, either in the periareolar region or in the inframammary region. The axilla is often an acceptable area for placing incisions in these women. The axillary skin usually heals better than other areas, and with less hypertrophy.
Aesthetic Procedures
A slender, angular body contour is most often seen in young nulliparous patients. In breast augmentation for women with this body type who are 5 feet to 5 feet 8 inches in height, weigh 45 to 54 kg (100–120 lbs) and who have a chest circumference of 32 to 35 inches, I usually find that implants ranging in size from 200 to 300 cc with a diameter of 11 to 13 cm provide attractive breasts in proportion to the patients’ bodies. Because their breast parenchyma and subcutaneous tissue are so thin, any capsular contracture or implant irregularity will be visible and palpable in the upper and lower poles of the breast. Therefore, I prefer to place the breast implants beneath the pectoralis major muscle to minimize the chance of seeing or feeling the implant, which may produce a rippled appearance. I also prefer the axillary incision, because it often heals better without leaving conspicuous breast scars, which pose possible problems, such as scar hypertrophy. Since these women may be athletic and have strong pectoralis major muscles, additional softening and expansion are obtained by releasing the lower and medial pectoral muscle origins and by dividing the medial pectoral nerve fibers to provide selective lateral pectoral muscle denervation, thereby reducing lateral tightness and muscle contractions over the breast implant.
Patients with this body configuration must have realistic expectations about what breast surgery can achieve. Their narrow chests and thin bodies limit the diameter and therefore the size of the breast implants that can be placed during breast augmentation. Breast implants are selected according to the base dimensions of the breast as well as chest wall circumference. Relatively large implants will extend the breasts too far laterally beneath the arms and create an unnatural upper pole fullness.
When these women have breast reduction procedures, which is unusual, their narrow chests and full breasts are prone to scars that can extend beyond the newly shaped and reduced breasts. Short-scar vertical reduction techniques are particularly useful in these patients.
Augmentation: Case Example
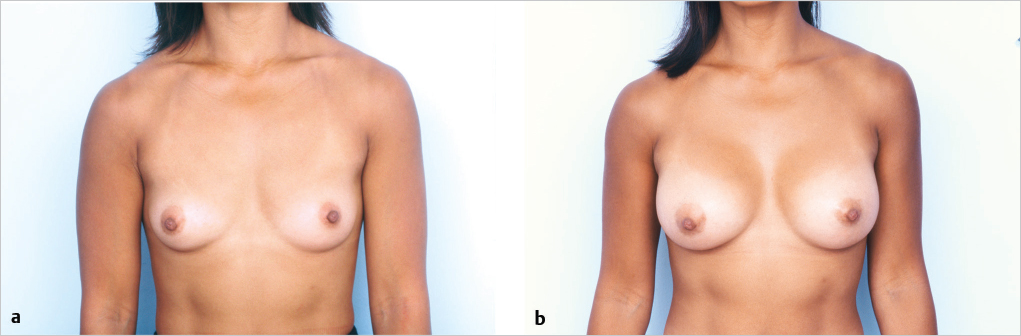
This 5-feet 4-inch, athletic, slim patient weighs 53.5 kg (118 pounds). She has well-developed pectoralis major muscles and small breasts. Her chest circumference is 34 inches. She was dissatisfied with her small breasts and desired a subpectoral breast augmentation with saline-filled implants placed through an inframammary incision. This was accomplished with 275 cc implants inflated to 300 cc with saline solution. She is shown 9 months after surgery with a pleasing result and soft breasts with grade 1 capsules (▶Fig. 2.12).
Related posts:
 5 Gene Mutations and Breast Cancer Risk: Overview and Management
5 Gene Mutations and Breast Cancer Risk: Overview and Management
 7 Technological Advances in Breast Surgery
7 Technological Advances in Breast Surgery
 10 Fat Grafting to the Breast in Prepectoral Breast Reconstruction—A Current Overview
10 Fat Grafting to the Breast in Prepectoral Breast Reconstruction—A Current Overview
 1 Anatomy, Physiology, and Aesthetics
1 Anatomy, Physiology, and Aesthetics
 8 Fat Grafting in Breast Reconstruction: The Data
8 Fat Grafting in Breast Reconstruction: The Data
 9 Fat Grafting to the Breast: Aesthetic and Reconstructive Applications
9 Fat Grafting to the Breast: Aesthetic and Reconstructive Applications
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


