2 Augmentation Rhinoplasty Using Silicone Implants
Pearls
For East Asian noses, major augmentation is frequently required for the nasal dorsum and the tip.
The silicone implant is widely used in Asian countries because it is easy to use, limitless in volume, cost-effective, and superior to the auto- or homograft from the aesthetic viewpoint.
There are two sources of problems related to the alloplastic implant. One is the problems inherent in the material itself, which can be minimized. The other is problems from technical or judgmental errors, which are more common and must be avoided.
Infection is a serious problem though uncommon. Thorough sanitization of the operation field, including the nasal vestibule and anterior nasal cavity, is important. Care should be taken not to tear the mucosal barrier using atraumatic techniques. Operation time should be reduced to decrease the chance of infection. The implant must be immersed in antiseptic solution before and after any manipulation.
Designing an implant must be individualized. The surgeon should have in mind the desired shape of the nose. Individual anatomic characteristics must be considered such as the nasofrontal angle, dorsal contour, and tip projection.
Proper selection of a tip technique is important. According to the tip technique, the design of an implant varies. The implant should be connected to the augmented tip smoothly and seamlessly.
Do not try to augment the tip with the implant. Unlike the relatively immobile dorsum, the tip is highly mobile. Therefore, only autologous cartilage must be used for the tip, with appropriate techniques to prevent extrusion and skin problems. An implant placed on the tip is aesthetically unpleasing because it always leads to a rotated tip with an unnaturally thick infratip lobule.
With the use of only autologous cartilage for the tip, skin problems are prevented and more natural outcomes are ensured.
Stacking of multiple layers of onlay grafts is commonly required for sufficient tip projection in Asians. The wing graft should be used in combination with the stacked onlay graft to prevent noticeability of the onlay graft and pinching deformity.
Complication rates of alloplastic implants are medically acceptable. Complications are more frequently the result of the surgeon’s technical and judgmental errors, rather than the fault of inherent characteristics of the material itself.
Introduction
The noses of East Asian people are different in many aspects from Caucasian noses. Augmentation rhinoplasty is one of the most common aesthetic procedures in Asian countries because of the relatively flat and wide Asian nose. However, augmentation rhinoplasty should be conservative, preserving the ethnicity to make the nose appear very natural and harmonious with other facial units. In Asian countries, augmentation rhinoplasty is not a major reconstructive operation. It is regarded as one of the uncomplicated common cosmetic procedures. It is often regarded as a trendy operation, and the aesthetic standard of patients is generally high. People want short recovery times and a quick return to the job, although major augmentation is frequently required.
In this situation, a practical and cost-effective option for a surgeon is rhinoplasty using an alloplastic implant. Amounts of autologous materials except for costal cartilage are limited for the usual large-volume augmentation. However, with the use of costal cartilage, economic and psychological burdens are heavy for patients. Other disadvantages include postoperative scarring on the chest, rigidity of the tip, prolonged operation time, and a long recovery period. In addition, the use of costal cartilage is not free of complications. Problems of warping and resorption are well known. Infection is rare but is possible. Therefore, costal cartilage is reserved as a last resort by many surgeons.
On the other hand, alloplastic implants are ready to use, easy to carve, varied in size, and superior to autologous materials from an aesthetic viewpoint. Also, they are not subject to resorption or warping. Among the most commonly used alloplastic materials are silicone, expanded polytetrafluoroethylene (Gore-Tex), and porous high-density polyethylene (Medpor, Stryker, Kalamazoo, Michigan).
Silicone is the most frequently used material in Asian countries. It is nonporous, in contrast to the other two materials, with no tissue ingrowth or vascularization seen after implantation. Because of its nonporous nature, it is nonadhesive to surrounding tissue and enclosed in a fibrous capsule. Also, it is free from deformation, easy to sterilize, and easy to remove when necessary. It is relatively cheap and available in a range of softness values.
Expanded polytetrafluoroethylene (ePTFE) is composed of nodules of Teflon interconnected by fibrils of polytetrafluoroethylene and has a microporous architecture, with pore sizes ranging from 10 to 30 mm. Its porosity makes it easily malleable and susceptible to longterm compression, resulting in volume decrease or deformation of the implant. Its hydrophobic and porous nature makes the sterilization process using an antiseptic or antibiotic solution difficult. Relatively high cost is another disadvantage. For the revision cases, sometimes it is very difficult to remove the previous ePTFE implant, especially when the implant is thin, and the duration of implantation is long. When the surrounding soft tissue is removed together with the implant, the resulting soft tissue irregularity is extremely difficult to repair.
Porous polyethylene (Medpor) consists of a continuous system of interconnecting pores of size 125 to 250 mm. The vascular and fibrous ingrowth leads to integration and stabilization of the implant. The tensile strength of the material is very high, contrary to the case for ePTFE. Because of its stiff nature, it should be used with utmost caution in mobile areas such as the membranous septum or tip.
Synthetic implants in rhinoplasty have been a topic of great controversy. In particular, silicone, which is the single most commonly used implant material in Asian countries, is a point of worldwide contention.1 Asian noses are considered more receptive to alloplastic implants because of their thick skin.2 This is true to some extent, but even thicker skin cannot resist longterm thinning, extrusion, inflammation, and infection. Therefore, proper techniques using an adequately designed implant must be executed.
When an experienced surgeon uses proper techniques, the complication rate for alloplastic implants is surprisingly low and in a medically acceptable range. Recent studies about the complication rates of alloplastic implants for augmentation rhinoplasty show that they are much lower than those in studies from the 1960s and 1970s.3 These changes are due to improvements in implant design, conservative surgical techniques, surgeons having more experience, and the use of softer silicone.
Patient Evaluation
The shape and profile of the nose requested by the patient, and their feasibility or desirability are discussed in this section. Advantages and disadvantages of using alloplastic implants and possible alternatives to alloplastic materials are also discussed.
Professional recommendations should be given to the patient after a thorough analysis of the face. The relationship of the nasal dorsum, tip, philtrum, lips, and mentum with the vertical facial axis should be investigated. In analyzing the face, any facial asymmetry must be noted and revealed to the patient before the surgery, because the augmentation rhinoplasty may worsen or accentuate a preexisting facial asymmetry. When the vertical facial axis is skewed or deflected, the augmented nose cannot be absolutely vertical and straight. In patients with significant facial asymmetry, it is better to augment the nose in a different vertical axis from the anatomic dorsum. In these patients, nasal bones on the two sides are frequently asymmetric in terms of the width and the slope. When the bony asymmetry is significant, the bottom of the implant is better carved asymmetrically accordingly.
Facial asymmetry commonly accompanies asymmetric nasal alae. Pre-existing alar asymmetry makes the nose look deviated even after augmentation to the correct axis. Asymmetric alar resection in these patients may not correct the problem satisfactorily. Alar asymmetry relating to facial asymmetry is difficult to correct because of its multidimensional nature.
A systemic examination of the nose is performed from top to bottom (Fig. 2.1). The relationship of the forehead with the nasal root is important for a successful dorsal augmentation. The Asian forehead is relatively flat and less protruding. Generally, Caucasians are more dolichocephalic and Asians are more brachiocephalic. Brow ridges in Asians are also not as prominent as in Caucasians. As a result, the nasofrontal angle in Asians is like a gentle and graceful curve rather than an angle. Augmentation rhinoplasty in Asians must preserve this gentle curvaceous transition from the forehead to the nasal dorsum. And the augmented nose must harmonize with the relatively flat forehead. Therefore, excessive augmentation of the radix area should be avoided in patients with a flat forehead. The proximal end of the implant should be carefully tapered to accommodate to this area and not be visible or palpable. Despite the retruded forehead, if the patient wants a substantial amount of dorsal augmentation, combined forehead augmentation should be considered. Forehead augmentation surgery is rarely performed in the West; however, it is a common surgery in Asian countries, using alloplastic implants or microfat injection.

In patients with excessive skin and soft tissue crowding in the glabellar and nasal root area, the brow lift should be considered. That is because augmentation rhinoplasty may make this area look heavier and thicker and may worsen the masculine look in these patients, leading to unsatisfactory outcomes. Aged patients tend to have brow ptosis and a thick soft tissue load in the glabellar area. Therefore, a combined brow lift surgery should be considered in aged patients and augmentation of the radix area should be minimized, focusing more on tip augmentation. However, even in young patients having a short distance from glabellar area to nasion, dorsal augmentation may further shorten the distance, making the nasal root area unnatural and flattened. Therefore, a combined brow lift surgery may be considered in these young patients also. The endoscopic brow lift is the best option for young patients considering the effect on the medial brow and minimizing postoperative scarring.
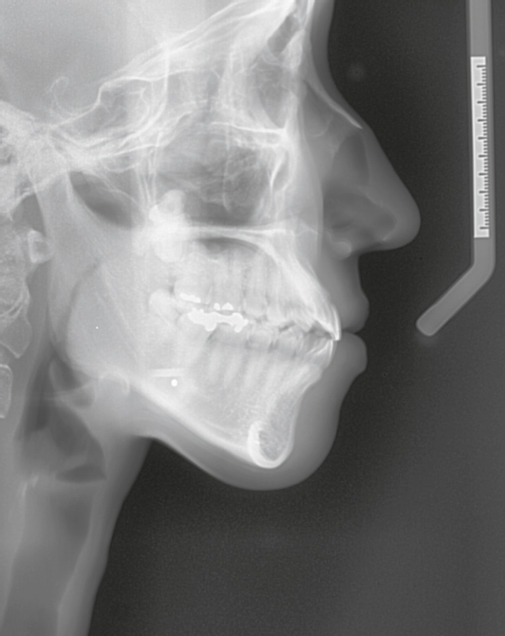
The glabellar and nasal root region shows a wide range of variation even in Asians. Therefore, the proximal implant should be carved carefully according to individual anatomy to fit in this area. Preoperative X-ray may be helpful for visualization of the bone and soft tissue anatomy of this area (Fig. 2.2). Examination by manual palpation of this area before or during the operation is also very important.
Careful dorsal examination precedes the design of an implant. The nasal bone is examined for its length, width, and asymmetry. Manual palpation along the dorsum is helpful in revealing soft tissue thickness, presence of hump, or dorsal irregularity.
Skin thickness of nasal tips is quite variable in Asians. For the thinskinned patients, visibility of grafts or the implant might be problematic. On the other hand, for the thick-skinned patients with bulbous tips, it is very difficult to obtain a fine definition of the tip.
Wide alae are common in Asians. For the enhanced outcome of dorsal augmentation, alar resection may be required in some patients. If alar asymmetry and asymmetric maxillary development are present, they are discussed with the patient, because it is unrealistic to try to make the sides of the alae completely symmetric. In patients with underdevelopment of the maxilla or premaxilla, paranasal or premaxillary augmentation may be considered as ancillary procedures of the augmentation rhinoplasty.
However, it should be taken into consideration that acute nasolabial angle is not uncommon in Asians. Some Asian noses are beautiful enough even with the acute nasolabial angle, and in some patients acute nasolabial angle is not a concern at all.
Patients with protruding lips can benefit from the combination of rhinoplasty, maxillary augmentation, and chin augmentation. This combination of surgeries will dramatically enhance the facial profile in selected patients.
Surgical Techniques
Skin Marking
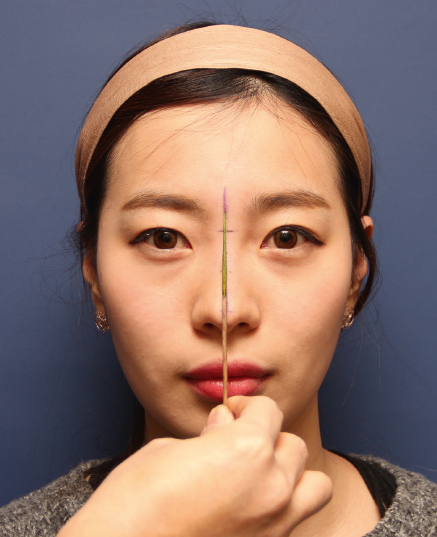
Skin marking for the augmentation must be done in the sitting position. Marking a vertical line for the dorsal augmentation is important, because frequently the glabella, nasal dorsum, and nasal tip are off the same vertical axis, and augmentation rhinoplasty may accentuate the deviated look of the nose.
Therefore, the surgeon must set a vertical line for the augmentation. The line that looks the straightest is carefully chosen for the line of augmentation (Fig. 2.3). When the dorsum and tip are vertically misaligned, usually a vertical line extended upward from the tip is more appropriate for the line of augmentation, rather than the line along the dorsum, although this is not always the case.
The nasal starting point is set and a horizontal line is marked, usually at the height of the ciliary margins. In general, when the patient wants a higher dorsum, the line may be drawn at the height of the supratarsal crease. When the patient wants a more natural look, then the line is drawn between the ciliary margin and the pupil. However, it is individualized according to the patient’s facial characteristics. This horizontal line also provides a landmark for the cephalic extent of the subperiosteal dissection.
Anesthesia and Positioning
The patient is put under anesthesia in a supine position and draping is done. Augmentation rhinoplasty using alloplastic implants is done under general anesthesia or intravenous anesthesia with sedation. When it is done under intravenous anesthesia, close monitoring of the respiration is crucial. Maintaining the oral airway during the surgery is required. Any blood or secretion in the oral and pharyngeal cavity is sucked out repeatedly using a suction catheter through the oral airway during the operation. To reduce the secretion, intravenous injection of glycopyrrolate before the surgery is recommended. Oxygen supplementation through the oral airway also can be helpful.
Preparation of the Implant
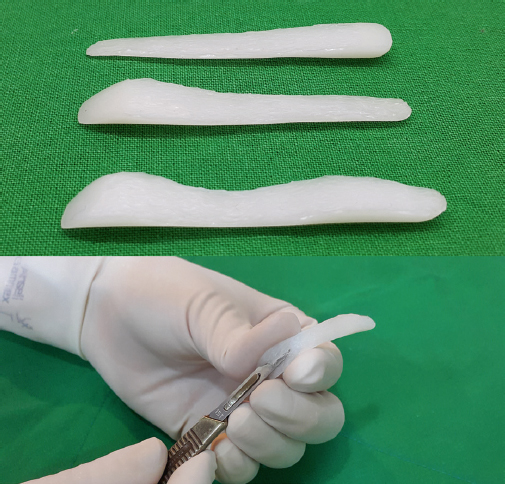
Before local anesthetic injection, an implant is prepared and tried on the dorsum (Fig. 2.4). The surgeon must check whether it is suitable for the desired height and desired nasal profile, whether it is well fitted for the nasofrontal angle, and the dorsal configuration. Then initial carving is performed using a no. 15 surgical blade before the surgery.

A correctly designed implant is crucial for a successful outcome. Any single implant must be customized according to individual anatomy. The thickness of the implant is decided first. Implants with 4 to 5 mm of thickness are most frequently chosen among the 2 to 10 mm thickness range. However the thickness is not uniform and varies along the dorsum after carving according to the individual’s anatomic characteristics. In general, when the nose is low in radix and the tip is well projected, the implant is carved proximally thick and distally thin. On the contrary, when the nose is adequately high in radix and the tip is low, the implant is carved proximally thin and distally thick. When a hump is present, the implant is often carved thinner in the rhinion area (Fig. 2.5).
The implant’s shape, especially the distal portion, is also variable according to the preferred tip augmentation technique.
The initially carved implant is immersed in antiseptic solution such as hypochlorous acid until its later use. The hypochlorous acid is suitable for this purpose because it is clear in nature and relatively less toxic, nonirritating, and potent.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


