5 Hump Resection
Pearls
Three common features of the Asian hump nose are small size, low radix/low dorsum, and underprojected tip.
Management strategy should be focused on achieving an ideal nasal profile and not on hump removal.
Obtaining a natural brow tip aesthetic line in the frontal view is as important as obtaining an ideal profile in the lateral view.
The amount of hump resection should be tailored based on the predicted amount of dorsal augmentation and tip projection.
Radix and tip augmentation often minimizes or obviates the need for hump removal.
Among various techniques for addressing hump nose, conservative humpectomy of the bony and/or cartilaginous hump, followed by radix and/or dorsal augmentation is the most commonly used method.
In case of a large hump, component hump resection with reconstruction of the rhinion using spreader grafts is recommended.
Complications of hump reduction include inverted-V deformity, dorsal irregularity, and nasal obstruction. These can be prevented by conservative hump removal and use of spreader grafts or camouflage grafts.
Introduction
Rhinoplasty is one of the most common facial plastic surgeries performed in Asia. Although the principles and goals may be similar, the actual execution is quite different from the Western version. Anatomic characteristics of the Asian nose coupled with differences in aesthetic standards demand that it be approached in a unique way. Numerous articles have been published highlighting these different approaches and techniques.1,2,3,4 Rhinoplasty among Asians involves peculiarities that distinguish the procedure from its Caucasian counterpart. Asian hump noses. In this chapter, characteristics of the Asian hump nose will be addressed with emphasis on surgical techniques commonly used to obtain reliable results.
Nasal hump surgery is commonly regarded as a “reduction” surgery in most Western rhinoplasty textbooks and is also referred as “reduction rhinoplasty.” The common goal of a hump nose surgery is to obtain a natural contour of the nasal dorsum through adequate dorsal reduction while dealing with the issues of an open roof. Although there are Asian patients who have large humps, most Asian hump noses differ from Western ones in that the size of the nasal hump is not big, and the nose is frequently associated with a relatively low nasal dorsum and under-projection or under-rotation of the nasal tip. Naturally, correcting a hump nose in Asians entails distinct differences both in concept and technique.
A small hump and the additional need for augmentation of the dorsum and the tip often minimize the amount of hump removal and sometimes obviate the need for resection itself. Profiloplasty instead of reduction rhinoplasty might be a more suitable word when dealing with
Patient Evaluation
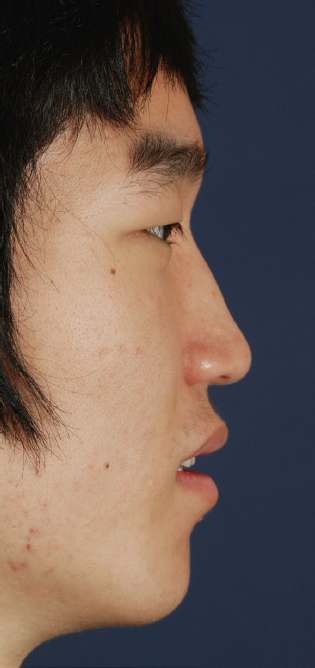
The key in preoperative planning is determining the ideal profile, which is somewhat similar to performing dorsal augmentation. There are two important points. The first is determining the level and height of the nasion. The level of the nasion, in other words, is the starting point of the nose. Differences in the starting point among different races have been emphasized consistently.5 Traditionally, the supratarsal crease has been considered the ideal starting point for Caucasians and the midpupillary line for Asians. However, there is a trend in which contemporary Asian patients are asking for a higher starting point. The authors consider the starting point in Asians to be somewhere in between the supratarsal crease and midpupillary line accounting for individual preferences (Fig. 5.1). The height of the nasion is usually determined by the nasofrontal angle. The ideal nasofrontal angle in Asians is around 135 degrees for males and 140 for females.

The next step is determining the desired nasal tip posture, which is done by considering nasal projection and rotation (nasolabial angle). The ideal profile can be achieved when a line is drawn from the nasion to the tip and the hump can be resected and/or the dorsum augmented as needed.
Other practical issues to consider include skin thickness, character of the hump, presence of deviation, and length of the nasal bones. The characteristics of the nasal hump are evaluated through careful visualization and palpation.
The hump may be generalized or localized. The generalized hump usually has a bony and cartilaginous component while a localized hump can be the result of a prominence of the nasal bone and/or upper lateral cartilage. A pseudo hump refers to the visual phenomenon of an accentuated height of the rhinion (resembling a hump nose), which can be caused by a deep radix and/or a depressed lower vault near the supratip (Fig. 5.2). Strategies in this situation should be focused on restoring support and augmentation instead of resection.
We usually stress the profile or oblique view when evaluating the hump nose patient. However, there are also salient features in the frontal view that we have to consider and correct to achieve a good result in hump nose patients. The frontal view is the most important view after all. Hump stigmas in the frontal view include unnatural brow tip aesthetic lines (narrowing, widening, break, etc.), light reflex in the area of the hump, and skin thinning with frequent hyperemia or discoloration. Obtaining a natural brow tip aesthetic line in the frontal view is as important as obtaining an ideal profile in the lateral view.
Surgical Techniques
It is important to emphasize again that surgical techniques of hump reduction are not that different from the Western procedures. However, the decision of undergoing reduction versus augmentation or redistribution is the key in managing hump noses in Asians.
Anatomic Consideration and Clinical Implication
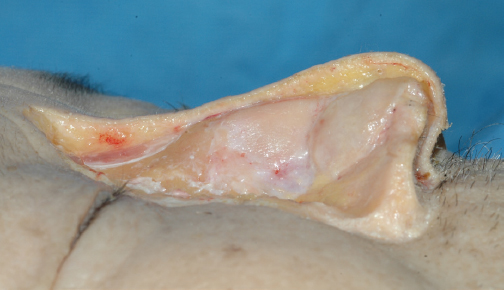
The dorsal skin is thickest in the nasion and thinnest in the rhinion (Fig. 5.3), resulting in a slight natural convexity in the rhinion area. There are two clinical implications related to this anatomic feature of the dorsum. First, when dissecting near the area of the rhinion or hump, a curved periosteal elevator comes in handy; and second, when reducing a hump, a flat dorsum is indicative of over-resection.
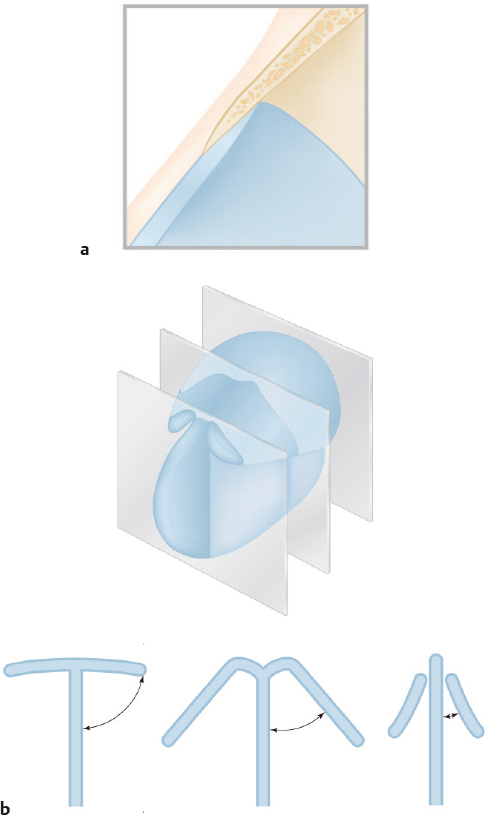
Anatomy of the rhinion area of the osseocartilaginous vault is another important point to understand when performing a hump reduction. There is a broad overlap of the nasal bones above and the septum and upper lateral cartilage (ULC) below (Fig. 5.4a). Many times it is sufficient to remove this bony hump until it reveals the underlying cartilage. There is a change in the shape of the dorsal septum and in its relation with the ULC as it progresses caudally from the bony junction—namely, from a broad “T” shape to a “Y” shape to an “I” shape (Fig. 5.4b). Resection of the dorsal septum while performing hump reduction will destroy this natural anatomy. Reconstruction with regard to the natural thickness of the dorsal septum will prevent aesthetic and functional complications such as the inverted-V deformity and nasal obstruction.
The Approach: Open versus Closed
Hump reduction itself can be performed with equal success via an endonasal or an open approach. Therefore, the choice of approach is usually dictated by the need for concomitant procedures to the dorsum and tip. The authors use the endonasal approach for a localized hump that does not need additional dorsal work other than augmentation (i.e., spreader graft) and needs only minor tip manipulation. A unilateral or bilateral intercartilaginous incision combined with a partial transfixion or hemitransfixion incision is preferred for accessing the dorsum, and a separate marginal incision is used for the tip.
An open approach is preferred in the majority of patients who have a generalized hump needing removal of the dorsal septal cartilage, have concomitant nasal deformities such as asymmetry or deviation, and need major tip changes. Although these maneuvers can be performed endonasally, the authors prefer the open approach because it provides better visualization and patient comfort in applying and securing grafts, thus ensuring a more stable and reliable result. The drawback of the open approach (i.e., a noticeable columellar scar) can be minimized by adhering to basic wound closure techniques.
Related posts:
 3 The Use of Costal Cartilage for Dorsal Augmentation and Tip Grafting
3 The Use of Costal Cartilage for Dorsal Augmentation and Tip Grafting
 4 Nasal Tip Modification in Asians: Augmentation and Rotation Control
4 Nasal Tip Modification in Asians: Augmentation and Rotation Control
 7 Correction of the Saddle Nose
7 Correction of the Saddle Nose
 6 Correction of the Deviated, Twisted Nose
6 Correction of the Deviated, Twisted Nose
 9 Aesthetic Rhinoplasty for Southeast Asians
9 Aesthetic Rhinoplasty for Southeast Asians
 10 Correction of the Short, Contracted Nose
10 Correction of the Short, Contracted Nose
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


