9 Aesthetic Rhinoplasty for Southeast Asians
Pearls
The bonycartilaginous structure of Southeast Asian noses is generally small in all dimensions, resulting in a relative abundance of skin and soft tissue. To achieve a longlasting effect, a strong framework is needed to counteract the forces of wound healing and the heavy skin and soft tissue complex.
Hanging ala of various degrees is often noted and can be easily corrected via “sail” excision. This procedure also improves columellar show.
The septal extension graft (SEG) is the workhorse in providing sturdy support to the tip.
The SEG may be inadequate as support in some cases. Additional grafts can be used to support the SEG (e.g., extended spreader and caudal margin extension grafts). Because of the paucity of septum that can be harvested, folded conchal cartilage attached beneath the SEG is often used.
Tipplasty is done before dorsal augmentation. After modifying the tip as desired, the dorsal graft is made to blend the new tip and the radix.
Among synthetic products for dorsal augmentation material, expanded polytetrafluoroethylene (ePTFE, popularly known as Gore-Tex) is preferred because it heals by tissue adhesion with no capsular formation. It provides a more natural look albeit with some undesirable potential complications such as deviation, visibility, and infection.
ePTFE in sheet form or preformed should be limited to a single piece if possible. Stacking of sheets may trap contaminants. The implant should be removed from its package only when it is time for dorsal augmentation to avoid prolonged air exposure.
ePTFE in sheet form is preferred for a shallow radix whereas the preformed type is preferred for correcting a deep radix.
The implant should be carved to follow the contour of the nose. The caudal end of the implant should be sutured to the dome to achieve a continuous structure of the dorsum and the tip.
A gap of space usually is left at the junction of the upper cartilage and lower cartilage after placement of the implant. This space should be filled with cartilage to prevent postoperative supratip depression.
Introduction
Noses of Southeast Asian peoples are generally small and short with a bulbous tip, thick skin and soft tissue envelope (SSTE) and a low nasal dorsum. Nasal bones may be wide at the attachment to the upper lateral cartilage. The tip is usually upturned. There is a certain degree of hanging ala, and columellar show is often deficient. The nasal framework is usually small, with a small nasal septum. The lower lateral cartilages are also small and weak, and the dome is ill defined with short medial crura. The anterior nasal spine and premaxilla are often underdeveloped.
Because of the features just mentioned, the surgery planned should include elongation and projection of the tip, augmentation of the dorsum, alar lifting and restructuring of the columella for a better columellar show and alar-columellar relationship, and augmentation of the premaxilla to improve the nasolabial angle. The most critical procedure is proper rotation and projection of the tip to a new position. As the septum is the most stable structure, the central part of the septum is harvested and is used for an extended septal support graft for fixation of the lower lateral cartilage to form a whole new tip. This maneuver also extends the columella for a better columellar show. The open approach is often used. The SSTE dissection is widely extended up to the piriform aperture laterally, nasal spine inferiorly, and glabella superiorly. The dissection plane should be below the superficial musculo-aponeurotic layer system (SMAS) on the upper and lower lateral cartilages, and below the periosteum on the nasal bone.
Patient Evaluation
“Thank you Dr. Yap for [the] nice work you did on my nose; however, I don’t like to look at myself in the mirror because I see a different person” (a female patient, 1 month postoperative).
Rhinoplasty remains the most common facial aesthetic procedure done in the Southeast Asian region. Patients should determine the right surgeon for themselves through thorough consultation with prospective surgeons. Prior to discussing the surgical plan, the patient should always be asked about the improvement sought for his or her nose. Computer simulation can be a dangerous tool because it may lead to future dissatisfaction resulting in arguments with the surgeon. It should be explained to the patient that improvements from the surgery largely depend on the existing structures. The aim of aesthetic rhinoplastic surgery is to improve the current appearance, not to achieve perfection. The majority of outcomes are good and fall within patients’ and surgeons’ expectations. However, there may be some cases where the outcome falls drastically short of expectations. This is often seen in noses with multiple aesthetic deficiencies (e.g., small nose, low bridge, bulbous upturned tip, retracted columella, retruded premaxilla, hanging ala, and wide alar base).
The patient should be aware that after the rhinoplasty surgery, there are a few possible reactions to the new nose. People who have frequent encounter with the patient (e.g., family members, office mates, and the patient herself) may find the change very obvious. Those who see the patient occasionally (e.g., high school and college alumni friends) may not be able to notice the difference; these people will generally comment that the patient looks more beautiful than before. People who had never met the patient prior to the surgery may not even notice that the patient has had surgery done on the nose.
Patients should be informed of the surgery in detail beforehand: extent of the surgery, duration of the surgery, type of anesthesia given, donor site, possible morbidity after harvest, and other pertinent points. Risks of the operation should be discussed thoroughly as well. Setting a realistic surgical goal is important. Patients are advised to keep an old picture of themselves close at hand for two purposes: for identification and to remind themselves of their previous appearance. Their new noses should be compared with their previous ones, not with other people’s noses.1
Surgical Techniques
Conchal Cartilage Harvest
Most Southeast Asian rhinoplasties need conchal cartilage for grafting since the harvested cartilage available from the septum is limited. This procedure is done before the actual rhinoplasty. Histologically, septal cartilage is a hyaline cartilage and is firmer; hence it is used as a support graft. Conchal cartilage, which is an elastic cartilage, is softer and is used mainly for contour, filler, and camouflage grafts.
The surgery can be done under general anesthesia or intravenous sedation. Following the usual aseptic technique, the face and the auricles are draped as a whole. Lidocaine 2% with 1:100,000 adrenaline is used as local anesthetic. Caution is advised toward the safe dose of lidocaine with adrenaline, which is 7.0 mg per kilogram of body weight.
The conchal cartilage is harvested either anteriorly, if only a small amount of cymba and cavum concha is needed, or posteriorly, if a bigger amount is needed. The anterior incision is done at the posterolateral portion of the cavum concha. The skin of the cavum concha is dissected above the perichondrium and elevated to the cymba concha. An incision in the cartilage is then made near the skin incision site, leaving 2 mm of cartilage beneath. Dissection is then performed at the posterior side, making sure that the perichondrium is preserved and remains attached to the cartilage. The conchal cartilage harvested should contain perichondrium on both sides to preserve the strength. It should be soaked in normal saline solution at all times before being fashioned as grafts.
For the posterior approach to conchal cartilage harvest, an incision is made between the sulcus and the helix. Dissection is above the perichondrium. Bleeders can be cauterized. To maximize the harvest of cymba and cavum concha, two or three hypodermic needles are used to pierce anteriorly at the edge of the conchal cartilage through and through. The cartilage is then incised and dissection is carried above the perichondrium anteriorly, preserving 5 to 8 mm of conchal cartilage near the external auricular canal.
Closure of incisions is a bit different. For incisions done anteriorly at the cavum the donor defect should have 2 mm of conchal cartilage below the site of skin incision. This will be helpful because it will serve as a platform for skin wound healing. Closure with a simple interrupted suture is done using nylon 5–0, including the cartilage to avoid a crumpled look at the incision site. A bolster suture is also applied to avoid hematoma formation. For a posterior incision, closure is done using nylon 5–0 vertical mattress sutures. Sometimes the harvest site of the cymba and cavum concha contracts, especially at the big auricle; to avoid collapse and contracture, a strip of cartilage between the cymba and cavum is preserved.
Alar Lift Surgery via Sail Excision
Hanging ala is common in Southeast Asian noses. Before the start of surgery the tip is manually pulled to its desired position to simulate counter-rotation and projection. Attention should also be given to the alar-columellar relationship. If there is a need for alar lifting it should be done as the initial procedure since the whole lower part of the nose is still mobile and will allow maximal flexibility in maneuvering the ala during marking, traction, excision, and suturing.
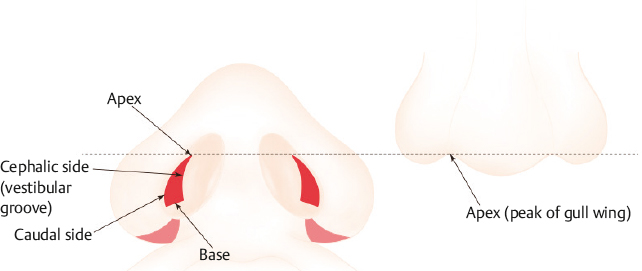
The alar rim can be lifted by excision of a triangular piece of tissue in the inner lateral vestibular skin (Fig. 9.1). The irregular triangular piece of skin tissue is shaped like the sail of a sailboat. The two sides are marked at the inner alar rim margin, and a skin groove in the lateral vestibule area is marked by the transition of thin vibrissae to thick vibrissae. The apex of the triangle is located at the highest curve in the “gull wing” on the frontal view. The alar rim skin is made to roll cephalically as a flap, thus lifting the whole alar rim. The defect is closed using nylon 6–0 simple interrupted sutures (Fig. 9.2).2

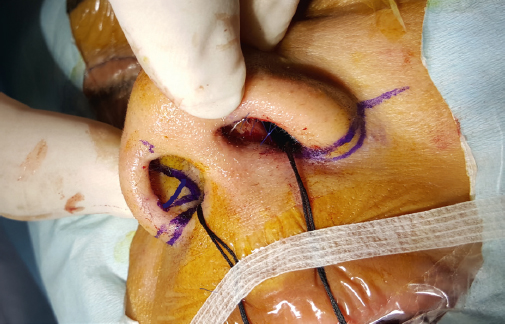
There are some instances where the alar base is lower than the columellar base. The alar lift surgery should be aggressive to lift the alar base as well. This procedure involves a radical “sail” excision by extending the incision inferiorly and posteriorly following the vestibular groove. The design of the extended sail excision is actually a small triangle inferior to the sail diagram; its apex is pointing inferior-posterior (Fig. 9.3). Closure is done via absorbable suture 6–0 simple interrupted at the sill area and nylon 6–0 simple interrupted at the rim (Fig. 9.4).

The Approach
Since the majority of Southeast Asian noses need structural modification, an open approach is preferred for better visualization. A marginal incision is first made. The columellar incision at the medial crura is made behind the skin mound and anterior to the hair-bearing area. Another incision is made 2 to 3 mm caudal to the edge of the lower lateral cartilage. The medial incision and the caudal marginal incisions are then connected maintaining 2 to 3 mm of skin. Maintaining a 2- to 3-mm vestibular skin allowance ensures good coaptation during closing with sutures.
Dissection of the lower lateral cartilage is approached at three sites: first at the medial crura, then at the lower lateral cartilage, and finally at the dome. A soft tissue dissection is done at the medial crura. The dissection of the lower lateral cartilage is done above the perichondrium. At this time a transcolummellar incision can be made and the domes are dissected away from the overlying skin and soft tissue envelope. The dissection of the lower lateral cartilage is carried superiorly and laterally up to the scroll junction of the upper lateral cartilage and the lateral ends of the lower lateral cartilage.
The dissection of the dorsum at the area of the upper lateral cartilage should take place beneath the SMAS. This is achieved by carefully applying blunt and sharp dissection at the dorsal septum near the anterior angle. Once the plane is identified at the dorsal septum, a blunt dissection is done lateral-ward until the piriform opening edge of the maxillary bone is reached. At this time the lower lateral cartilage should be fully mobile for tip repositioning.
The upper dorsum comprises the nasal bones. The plane of dissection is subperiosteal. Use a sharp periosteal elevator, and take care to avoid injury to the dorsal nasal nerve that exits 5 to 6 mm lateral to midline between the nasal bones and upper lateral cartilage (Fig. 9.5).
Membranous Septum Dissection: Two Points in a Plane Determine a Line
The membranous septum should be opened for access to the caudal edge of the septum. The dissection also frees the medial crura and footplate for tensionfree tip repositioning and columellar show.
A safe approach to split the membranous septum is following the geometric rule of “two points in a plane determine a line.” Point A is the anterior angle of the septum and point B is the footplate. The “plane” is the membranous septum. After identifying the anterior angle of the septum, the fibers of the opposing medial crura are dissected via blunt dissection up to the anterior nasal spine. This maneuver exposes the footplates. A sharp dissection of the membranous septum between the anterior angle of the caudal septum (point A) and the footplate (point B) is now performed until one reaches the caudal margin of the septum.3
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


