7 Correction of the Saddle Nose
Pearls
Evaluation of the degree of septal support is the most important step in preoperative planning in a patient with saddle nose deformity. This is because a saddle nose is often due to a damaged cartilaginous septum.
Class 1 saddle nose has good cartilaginous septal support with a minor supratip depression. This can be easily corrected by cosmetic dorsal camouflage.
Class 2 saddle nose has moderate loss of septal cartilaginous support with moderate dorsal depression, which can be managed by reinforcement and reconstitution of the septum and/or dorsum.
Class 3 saddle nose has severe loss of septal cartilaginous support with a moderate to severe dorsal depression. Subtotal septal reconstruction with costal cartilage should be administered to correct this saddle deformity.
Class 4 saddle nose has severe loss of septal cartilaginous support with both bony and cartilaginous dorsal depression, in which case the dorsal framework from the radix to the tip needs to be totally reconstructed with costal cartilage.
Correction frequently requires straightening or reconstituting the Lstrut. A stable L-shaped strut of septal cartilage to the nasal spine is crucial to support the upper and lower lateral cartilages to maximize the results in creating a straight and functional nose.
Introduction
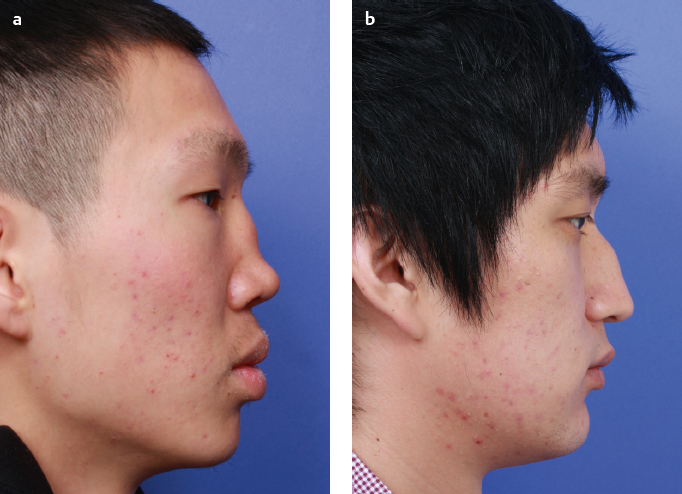
Nasal deformities affecting mainly the lower twothirds of the nose due to the loss of septal height and tip support are defined as “saddle nose” deformities (Fig. 7.1). A saddle nose was first described by John Orlando Rose in 1887 as a “pug nose.” A pug is a kind of canine with an almost complete absence of a snout or nasal dorsum. The depression noted on the middle vault of the nasal dorsal surface resembles the saddle of a horse—hence the term saddling.
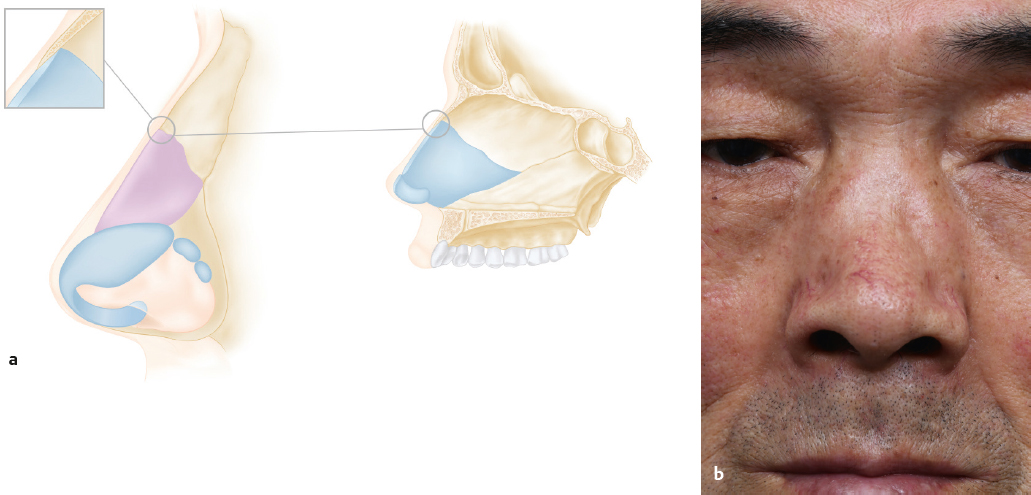
Complex deformities of the nasal septum can have both an aesthetic and a functional impact on a patient’s nose. If there is a severe compromise of the cartilaginous septal integrity with subsequent loss of middle vault support by the septum, dorsal depression develops, followed by loss of tip definition and other associated features (Fig. 7.2 and Fig. 7.3).1,2 This kind of nasal deformity is often very distressing to the patient as the deformity is obvious and unattractive. Functionally, patients can complain of nasal obstruction due to the collapse of the internal nasal valve.
While saddle nose deformity is caused by the loss of septal support and shows a true loss of dorsal height, a pseudo saddle is a relative depression of the supratip region caused by a hump nose. For correction, a saddled nose requires the reconstruction of the scaffold of the dorsum—for instance, the septum—but a pseudo saddle needs to have the hump resected to allow the supratip region to look normal again.
Anatomic Considerations
Saddling of the nose is essentially caused by the loss of nasal septal support for the dorsum of the nose. Support of the nasal dorsum is provided by the cartilaginous and bony structures involved in nasal projection. The nose is divided into the upper, middle, and lower thirds, commonly known also as the upper, middle, and lower vaults.
The upper third is supported by the pyramid of the nasal bone. The interlocking of the quadrangular cartilage with the nasal bone forms the keystone area, which is the key area that should be preserved to prevent the collapse of the saddling of the dorsum and creation of the inverted-V dorsal deformity (Fig. 7.2). The quadrangular cartilage is the single most important cartilage that supports the lower two-third of the nose, including the nasal dorsum and the paired upper and lower lateral cartilages. Most of the etiologies mentioned above disrupt the integrity of this cartilage to cause saddle nose deformity. Therefore, correction of the saddle nose deformity usually, if not always, centers on reconstructing and reestablishing the strength of the quadrangular cartilage.
The paired upper lateral cartilages constitute the lateral side of the middle vault. The angle formed by the upper lateral cartilage and the nasal septum is the internal nasal valve. Since the strength of the upper lateral cartilages relies heavily on the nasal septum, loss of support in the nasal septum will result in collapse of the internal nasal valve. Rectifying a saddle nose without addressing this area will leave functional problems such as nasal obstruction.
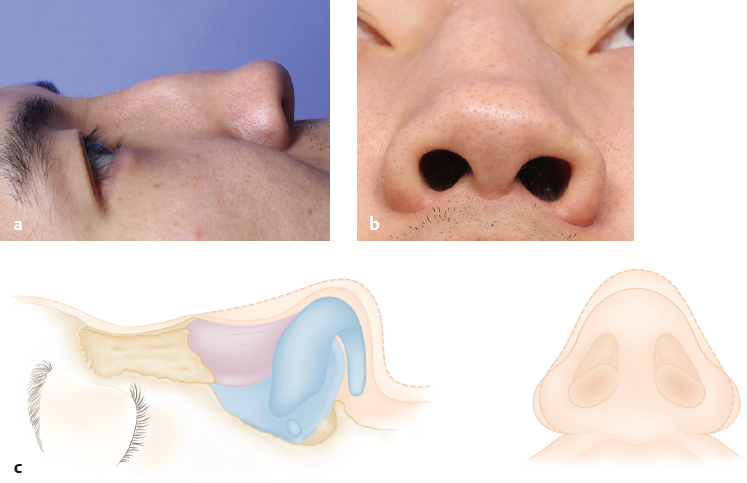
Lower lateral cartilages define the tip and are also supported by the septal cartilage. Loss of height and width of the septal cartilage will cause misalignment of the lower lateral cartilages, resulting in loss of tip definition, tip ptosis, cephalic rotation, and retrusion of the columella (Fig. 7.3).
Etiology of Saddle Nose
In recent years, most saddle nose deformities have come from trauma, and from nasal surgeries, including septoplasty and rhinoplasty. Inflammatory diseases were common causes in the past.2,3
Trauma
Trauma may physically destroy the cartilaginous or bony structures of the dorsum and the nasal septum. Posttraumatic hematoma in the nasal septum may be a cause of septal destruction or perforation due to hematoma organization and resorption or infection and abscess formation secondary to the hematoma. Saddle deformity after trauma is usually accompanied by a deviated nose, septal deviation, and nasal valve collapse.
Iatrogenic Factors
Saddle nose could also be a secondary deformity due to resorption or a problematic implant used in nasal septum or nasal dorsum reconstruction, especially if the keystone area is inflicted during septoplasty or rhinoplasty. Over-resection of the quadrangular cartilage causing weakening of the septal cartilage during surgery could result in saddling. It is therefore important to preserve at least 10 mm of the dorsal and caudal part of the quadrangular cartilage when cutting the nasal septum. Sometimes saddling caused by nasal surgery will not be apparent immediately after the surgery but will slowly manifest over time.
Systemic Diseases
Systemic diseases such as granulomatous diseases and autoimmune diseases may compromise the integrity of the nasal supporting structures and cause saddle nose deformity. Granulomatous diseases such as Wegener’s granulomatosis; infection such as leprosy and syphilis; and autoimmune diseases such as relapsing polychondritis, sarcoidosis, and Crohn’s disease may destroy the septal cartilage along the disease process due to chronic inflammation.
Malignancy
NK-T-cell lymphoma, squamous cell carcinoma, malignant mucosal melanoma, adenocarcinoma, minor salivary gland tumors, and metastatic lesions are just some of the malignancies known to destroy structures that provide dorsal support to the nose, inducing saddling.
Vascular Ischemia of the Nasal Septum
A classical cause of saddling is septal perforation due to cocaine abuse, secondary to the repeated and sustained action of sucking in cocaine through the nose. Ischemia to the nasal septal vasculature will eventually result in a large septal perforation, especially in the cartilaginous portion, and collapse of the dorsum. Similar assault to the nasal septum could be caused by prolonged use of oxymetazoline nasal spray or other vasoconstrictive agents.
Patient Evaluation
Assessment of the Patient
History of trauma, previous surgery, systemic diseases, use of a topical vasoconstrictor, and cocaine abuse should be elicited. Details of previous surgery and the surgical manipulation could give insight into the available remnant cartilage and structural deficiency that has resulted in the saddling.
Proper consultation will start with thorough anatomic evaluation for factors that could affect the nasal deformities. Careful palpation and inspection can reveal the relation among the structural deformities including the nasal septum, cartilaginous and bony dorsum, tip, nasal valve, and turbinate. The resistance and resilience of cartilage should be evaluated in accordance with the strength and shape of the tip and caudal septum. Description of the nose should be made from all angles. In the photos, the lateral nasal length, the degree of depression, the presence of columellar retraction, and the degree of tip rotation/derotation should be carefully noted.
In general, saddle nose shows a broad dorsum, wide base, and inverted-V deformity in case of keystone area damage on frontal view. Lateral and oblique views reveal lower profile dorsum, saddling, retracted and short columella, low projection of the tip, and cephalic rotation in severe cases. The basal view reveals a low tip, round and flared nostrils, short columella, and wide base (Fig. 7.3). The presence of a dorsal hump that gives rise to a saddled appearance must not be confused with pseudo saddle.
Nasal cavity evaluation should be performed also. Septal evaluation is critical for evaluation of traumatic deformed nose. Sometimes overlapping fractured cartilage and replacement of scar tissue in the affected cartilage or fracture lines can make septal mucosa elevation difficult. Nasal valve obstruction should be assessed clinically followed by acoustic rhinometry or rhinomanometry tests, which could document and assess the level of obstruction prior to the surgery. The availability of septal cartilage, septal perforation, and any deviation should be carefully noted during endoscopic examination to facilitate planning of the surgery. If endoscopic findings suggest other medical problems causing the loss of septal cartilage, be sure that the patient is screened for autoimmune or infectious diseases, as previously discussed, before the repair is planned.
After external and internal examination, discussion about the preferred sources of grafts is mandatory. Patients should be given the choice of autologous, homologous, or synthetic grafts depending on the circumstances after the pros and cons of each option have been discussed. Rib cage views could be necessary if rib cartilage grafting is planned.
Most patients want to correct the both cosmetic and functional problems. On some occasions, a patient may request a higher projection and a better-defined tip compared with the premorbid nose. Therefore, a realistic consultation should be carried out with the patient.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


