10 Correction of the Short, Contracted Nose
Pearls
Repeated rhinoplasties causing trauma to the skin, soft tissue, and cartilages, implant use over the lower lateral cartilage causing pressure necrosis, and over-resection of cartilages will ensue scar contracture with resultant short, contracted nose.
With every effort made to correct the deformity, often the postsurgical contracted, short nose cannot be elongated to a level equal to patient expectations. It is crucial to have an adequate consultation before surgery.
The strategies for correcting secondary short nose deformity include skin envelope release through wide undermining, elongation and derotation of the tip component, augmentation of the dorsum, and use of composite graft material to fill the gap between the elongated skin envelope and the underlying vestibular skin.
In most cases of short nose correction, costal cartilage is necessary for structural support and onlay grafting.
A septal extension graft strongly supported with bilateral extended spreader grafts using rib cartilage is the key structural foundation on which the lower lateral cartilage can be repositioned.
An end-to-end type septal extension graft has the advantages of aligning the center into midline and avoiding caudal septal deviation compared with the overlapping type.
Various onlay grafts over the repositioned lower lateral cartilage can help to lengthen or augment the tip.
A chondrocutaneous composite graft taken from the cymba concha is often needed to fill the gap between the lengthened skin envelope and the vestibular lining.
A staged operation or even a forehead flap will be necessary if the skin shortage is severe in an extremely contracted or destroyed nose.
Warping of the rib cartilage used as a dorsal onlay graft can be minimized with proper techniques but is not completely avoidable. It can be corrected with revision surgery after full-blown warping has occurred.
Introduction
The short nose, the so-called snub nose, is objectively defined as having a decreased nasal length with an abnormally increased nostril show from the frontal view (Fig. 10.1). The tip is rotated cephalically with a more obtuse nasolabial angle on the lateral view. The astute surgeon should also note that a deep nasofrontal angle contributes to the subjective appearance of a short nose, especially when combined with an obtuse nasolabial angle.

The short nose can be congenital in origin, but is usually acquired secondary to trauma or from a previous rhinoplasty. In postsurgical cases, over-resection of the lower lateral cartilage is a frequent predisposing factor in Caucasian rhinoplasty. On the other hand, in East Asian patients, a postsurgical short nose deformity arises from different mechanisms.
The exact pathogenesis of short nose developing after rhinoplasty using an alloplastic implant is unknown yet but capsular contraction around the implant used for dorsal augmentation, lower lateral cartilage necrosis by longterm pressure from implants, chronic inflammation, and scar contraction from multiple rhinoplasties are thought to be possible etiologies. This condition is rather common in patients with weak lower lateral cartilages who had multiple rhinoplasties with silicone implantation.
Techniques to lengthen the nasal tip are oriented to adding cartilage grafts to the caudal septum to caudally rotate the tip, securing spreader grafts to a columellar strut, tip grafts of various shapes, and placement of radix grafts to elevate the nasion.1 Most postsurgical contracted noses have both structural problems, such as weak alar cartilage and decreased skin compliance caused by a damaged skin–soft tissue envelope. Because of these features, short nose correction has become one of the most difficult procedures in rhinoplasty.
Patient Evaluation
The patient’s history of previous surgery needs to be questioned very thoroughly. Dates and number of surgeries, surgeons’ names, materials used, techniques used, and any specific reasons for multiple surgeries, including complications, need to be evaluated. Thorough data are important in planning surgery.
The external nose is palpated carefully to evaluate the skin, underlying bone, and cartilage. When the skin is too thick or has a scar that decreases its mobility, the amount of lengthening of the nasal tip can be limited. A sense of the adequacy of skin mobility can be gained by pressing down on the skin and pulling on it (Fig. 10.2). Extremely thin and adherent skin may cause difficulty in undermining and will raise the possibility of skin damage. Every effort should be exerted not to damage the skin in this case.

The nasal cavity, especially the septum, should be thoroughly evaluated. In revision cases, there is a high chance that septal cartilage has already been used in the previous surgery and not infrequently there are septal perforations. The intact-looking septum needs to be carefully palpated with cotton tips, and often a thin, membranous posterior septum with missing cartilage can be felt. In extreme cases, the caudal septum is missing, causing severe shrinkage and contraction of the tip. In these cases, lengthening of the nose is possible only after the caudal septum is restored.
Elongating a short, contracted nose is a very difficult job, and even with extensive structural groundwork, the nose can be lengthened only by 3 to 4 mm. Therefore, the limitations of the surgery need to be explained thoroughly to the patient and a reasonable surgical goal needs to be set. Often the patients tend to have unrealistic expectations, such as that the nose will look normal and more beautiful compared with its preoperative status. Realistic patient expectations and a reasonable surgical goal considering the nasal status and the surgeon’s experience are the most important factors in the success of the surgery.
Surgical Techniques
Strategies for Correction
If the degree of cephalic rotation is mild and the tip support is strong, adding cartilage grafts on the tip and the dorsum may give some degree of caudal rotation of the tip and the illusion of nasal lengthening by dorsal augmentation. In a very short nose caused by severe cephalic rotation of the tip-defining point, merely raising the nasion with an implant on the nasal dorsum, or pulling down the tip-defining point slightly by placing a graft on the nasal tip has limited lengthening effect. More radical reorganization and repositioning of the lower nasal framework and skin envelope are necessary. Proper surgical technique is chosen considering the prior operative history, patient expectations, the degree of cephalic rotation of the nasal tip present, skin mobility, and the amount of available cartilage for use as grafts.
In most postsurgical contracted, short nose, caudal rotation of the tip-defining point and raising the nasion superiorly are two key surgical goals. Caudal rotation of the tip-defining point is obtained by caudally readjusting the lower lateral cartilage on the septal extension graft with or without additional tip onlay grafts (Fig. 10.3). To caudally rotate the tip without losing projection, a firm structural support reinforcing and lengthening all three legs of the “tripod” of the nasal tip is needed.
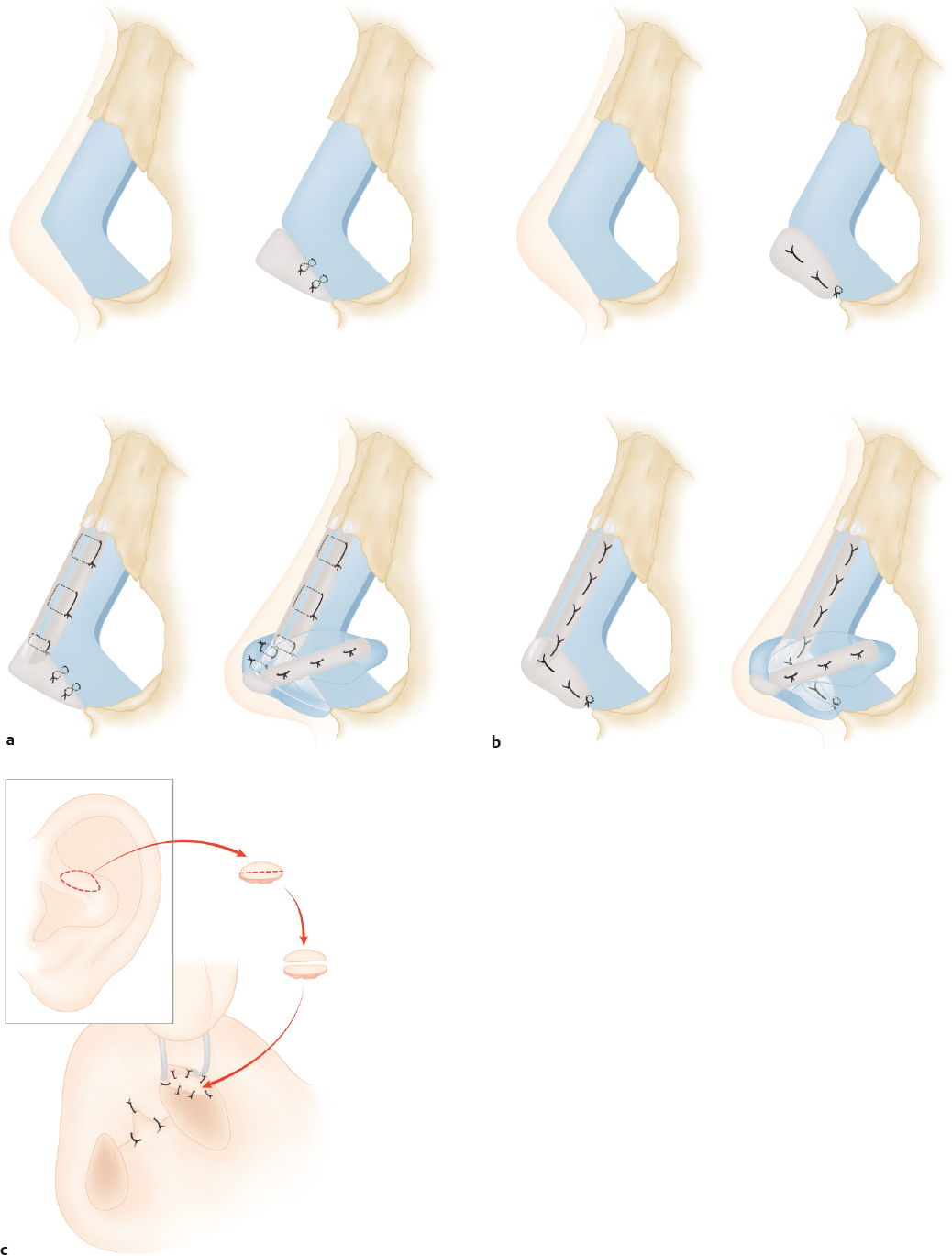
When the central part of the nose (i.e., the columella and the tip lobule) is lengthened with a septal extension graft, the lateral crus moves vertically upward and so does the alar margin. The alar margins also need to be lowered to create a more balanced nostril after the placement of the septal extension graft. Slight imbalance can be adjusted with a lateral crural onlay or strut graft. Placing a long lateral crural strut graft–lateral crural complex into a pocket made in the piriform aperture may lower the alar margin in the thinskinned Caucasian patient, but this maneuver is not as effective for East Asians, who have thicker skin. In most cases, the stiff and inelastic skin envelope and deficient vestibular skin are the most commonly encountered limiting factors during the lowering procedure of the alar rim. The author prefers to use conchal composite grafts from the cymba concha to fill the gap between the elongated skin envelope and the deficient vestibular mucosa, at the same lowering the alar margin (Fig. 10.3c ).
Many Asian patients want tip augmentation even in a situation that calls for the correction of short, contracted nose; however, it is not easy to get both an improved projection and caudal rotation of the nasal tip. When sufficient projection is achieved, the nose is found to be adversely rotated cephalically. Conversely, correcting the short nose with only caudal rotation usually ends in insufficient tip projection. Thus, an adequate compromise between augmentation and caudal rotation of the tip needs to be found.
Graft Material Harvesting
In most cases, the septal cartilage or conchal cartilage is insufficient and costal cartilage is used. Before deciding to use costal cartilage, it is prudent to check the rib series for possible calcification of the cartilage. Not infrequently, young female patients have severe calcification of the costal cartilage.2 Calcification makes harvesting and carving of the cartilage difficult. If the cartilage is totally calcified, it is very difficult to use as graft material.
The costal cartilage graft is harvested mostly from the sixth or the seventh rib for use in rhinoplasty. In female patients, the incision is placed just above the inframammary crease for better cosmesis (Fig. 10.4). In male patients, the incision is made directly over the chosen rib. The proper cartilage is located after palpation, and the costochondral junction is confirmed by serial probing with a 26-gauge needle. Marking is usually 1.5 to 2.0 cm in length in thinskinned patients and 2.0 to 2.5 cm in thick-skinned patients. A local anesthetic is infiltrated at the incision site. Ten minutes after injection, the skin and subcutaneous tissue is incised with a no. 10 blade. The subcutaneous fat is alternately separated and retracted using Senn retractors until the fascia and the external oblique muscle layer are exposed. The fascia is then incised and the muscle fibers separated with Kelly or mosquito forceps. To adequately expose the surgical field, the muscle layer is retracted with an Army-Navy retractor for better visualization, instead of cutting with a Bovie, to minimize postoperative pain. The perichondrium and the rib are sufficiently exposed after retracting the soft tissue and muscle.

Two parallel incisions are made on the perichondrium of the rib along the superior and inferior borders, leaving the central strip of perichondrium on the anterior surface intact. Following this, several cuts are made perpendicular to the longitudinal incision to facilitate circumferential reflection of the perichondrium, which is then dissected from the rib with a Freer elevator. The straight portion of the rib is often found to be of insufficient length for dorsal implantation, necessitating extension of the cartilaginous cut up to the synchondrosis portion to obtain a longer piece of cartilage.
Harvesting is facilitated if an anterior cut is made at the medial end of the cartilage before completing the dissection of the posterior surface of the costal cartilage. The perichondrium of the posterior surface of the rib is dissected off as much as possible with a curved elevator. The costochondral junction is identified visually or with the help of a 26-gauge needle and the cartilage cut is made. There is a great risk of injuring the underlying pleura if a complete cut is made using the no. 15 blade; thus, the final cut is completed with the Freer elevator to prevent such an injury. After the lateral cut, a small two-prong retractor is used to pull up the costal cartilage to expose the posterior surface and the dissection is continued medially. After complete dissection of the posterior perichondrium, the costal cartilage is separated at the medial cut and delivered out.
A 3- to 4-cm length of costal cartilage is typically harvested. The central strip of perichondrium is dissected and preserved for later use. The harvested costal cartilage is soaked in warm saline to assess for and induce warping prior to carving. Testing for air leakage from the pleura is performed by filling the dissection pocket with saline and then initiating positive-pressure hyperventilation. If no air leakage in the form of bubbles is evident, the donor site is packed with antibiotic-soaked gauze until the operation is completed. Additional costal cartilage can be harvested during the operation or the cartilage remaining after grafting can be reinserted and preserved under the muscle layer for use in future revision surgery. If air leakage is noted, a Nélaton catheter is inserted at the leakage site and sutured in a pursestring manner. After tight closure of the subcutaneous and skin wound, the Nélaton catheter is removed while simultaneously administering intense positive-pressure hyperventilation.
The separated muscles are tightly approximated to diminish postoperative pain and the wound is closed layer by layer using 4–0 Vicryl sutures. No drain is inserted. The skin margins are often bruised with discoloration due to excessive retraction, and these are trimmed and sutured with 6–0 nylon and a compressive dressing is applied. The nylon sutures are removed on the seventh to tenth postoperative day. Ordering a chest X-ray to check for pneumothorax immediately after the operation is not obligatory if the surgeon is confident that there was no air leakage through the harvest wound. If the patient presents with signs and symptoms of pneumothorax following surgery, then a chest X-ray is warranted. Rarely, a pneumothorax can occur even though there was no leakage during the intraoperative checking. Mild pneumothorax can resolve spontaneously with a serial followup of chest X-ray; however, a chest tube is inserted to expand the collapsed lung in nonresolving or severe cases.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


