18 Velopharyngeal Dysfunction
Summary
Velopharyngeal dysfunction (VPD) describes the improper closure of the velopharyngeal valve leading to abnormal speech production including hypernasality and nasal air emission. VPD can be divided based on its underlying etiology into velopharyngeal incompetence (abnormal neurophysiology and movement), velopharyngeal insufficiency (VPI; abnormal anatomy), or velopharyngeal mislearning (articulation error). VPI frequently results from overt cleft palates, submucous cleft palates, or large palatal fistulas of the hard palate. Nonoperative management of VPI includes speech therapy and prosthetics such as palatal lifts and palatopharyngeal obturators. However, the primary treatment of VPI is surgical.
18.1 Introduction
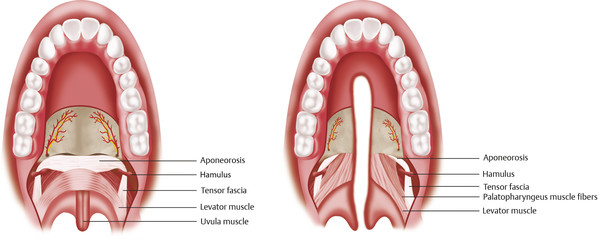
The velopharynx is composed of the soft palate, or velum (from Latin which means veil), and pharynx. The velopharynx is made of five muscles: the levator veli palatine (LVP), the tensor veli palatine (TVP), the palatoglossus, the palatopharyngeus, and the musculus uvulae. The superior pharyngeal constrictors and the salpingopharyngeus contribute to pharyngeal wall movement. The pharyngeal plexus (9th and 10th cranial nerves (CN IX and CN X)) innervates all of these muscles, except for the TVP, which is innervated by CN V (Table 18‑1).
Closure of the velopharynx separates the oral and nasal cavities during both speech and swallowing. Opening of the velopharynx is required for the consonants “m/n/ng.” Closure of the velopharynx is needed for the normal production of all other sounds in the English language. During closure of the velopharynx, the palate is pulled superiorly and posteriorly by the LVP and makes contact with the posterior pharyngeal wall at a condensation of the superior pharyngeal constrictors known as Passavant’s ridge. Normal speech requires the rapid movement of the velopharynx in order to generate both oral and nasal sounds.
Velopharyngeal dysfunction (VPD) in individuals with cleft palate can result in audible stigmata, with hypernasal speech, nasal air emissions, and inappropriate compensatory articulation errors. The incidence of VPD after palatoplasty has been reported from 5 to 40%. The impact of VPD is profound, and has the potential to affect social function and self-image.
Although the most common cause of VPD is anatomic/structural abnormalities, any pathology that results in abnormal velopharyngeal function can cause VPD. Previous classification of VPD was filled with confusion. The etiology of VPD was categorized as anatomic, iatrogenic, or neurogenic. VPD was further divided into whether it resulted from structural, functional, mechanical, or dynamic palatal dysfunction. More recently, VPD is now classified into three major diagnostic types: velopharyngeal incompetence (abnormal neurophysiology), velopharyngeal insufficiency (VPI; abnormal anatomy), or velopharyngeal mislearning (articulation errors; Table 18‑2).
18.1.1 Velopharyngeal Incompetence (Abnormal Neurophysiology)
This type of VPD is given to velopharyngeal pathology of unknown origin or pathology secondary to abnormal neurophysiology. It is important to note that in velopharyngeal incompetence, no underlying anatomical abnormality is present. The neurophysiological abnormalities associated with velopharyngeal incompetence can be caused by underlying intracranial processes, acute cerebrovascular injuries, palatal paralysis, or neurological injuries to the pharyngeal plexus. Velopharyngeal incompetence may also be associated with congenital neurologic conditions such as muscular dystrophy, hemifacial macrosomia, or cerebral palsy. The clinical manifestation of velopharyngeal incompetence is similar to other types of VPD but also presents with weakness, paralysis, or incomplete coordination of the velum and pharyngeal musculature, resulting in hypotonia, dysarthria, and loss of protective reflexes (i.e., gagging and swallowing).
In addition to neurophysiological abnormalities mentioned above, VPD can also present in patients with motor speech disorders, or apraxia. Since voluntary action of the velopharyngeal valve is mediated by coordinated signals from the motor cortex to the velopharyngeal musculature, it is not surprising that patients with apraxia can display abnormal coordination of the velopharynx during speech sound production.
18.1.2 Velopharyngeal Insufficiency (Anatomical Abnormalities)
The second major type of VPD is VPI. This categorization is given to VPD cases that are the result of structural or anatomical velopharyngeal pathology. VPI more commonly results from congenital abnormalities such as cleft palates, submucous clefts, or palatal fistulas (Fig. 18‑1). These congenital conditions are associated with gross tissue deficiency at the level of the velum and pharyngeal walls, and therefore limit velopharyngeal valve competence. Additionally, since velopharyngeal closure is largely a function of the ratio of the pharyngeal depth to palatal length, patients with disproportionally shorter palates or long pharynxes may also demonstrate incomplete closure of the velopharyngeal valve. Not only can VPI result from gross tissue deficiencies, or abnormal structural proportions, but it can also arise from congenital soft-tissue disturbances that produce mechanical dysfunction of the velopharyngeal valve. For example, hypertrophied tonsils can mechanically interfere with closure of the velopharyngeal valve and therefore cause VPI.
Lastly, VPI can stem from iatrogenic causes such as gross tissue deficiency secondary to tumor resection, trauma reconstruction, or adenoidectomy. Since removal of hyperplastic adenoids is a common treatment for children with airway obstruction or chronic otitis media, adenoidectomy can commonly cause VPI. Conversely, procedures that increase the soft-tissue bulk of the velopharynx can also cause VPI. For instance, excessive soft tissue at the nasopharynx level as a result of a wide pharyngeal flap may limit apposition of the velum to the pharyngeal walls.
18.1.3 Velopharyngeal Mislearning
Patients with this type of pathology appear to have normal anatomical, neurogenic, and physiological velopharyngeal valve competency. However, these patients exhibit phoneme-specific nasal emissions; oral consonants are replaced by nasal airflow. Commonly, these patients display nasal emissions with only a select set of sounds such as CH, SH, Z, and S.
18.2 Diagnosis
Evaluation of VPD is necessary in order to identify the degree of dysfunction, the reason for the dysfunction, and to determine a course of appropriate treatment. Evaluation should be completed by a multidisciplinary team including a speech-language pathologist with training, knowledge and experience specific to the evaluation and treatment of VPD. Evaluation includes auditory-perceptual and instrumental assessments.
18.2.1 Perceptual Evaluation
Resonance
Resonance must be evaluated in speech. Resonance is a phenomenon that can only be perceived on vowels and voiced consonants. It is based on the amount of energy present in the oral cavity and/or nasal cavity. Hypernasality consists of too much energy in the nasal cavity on sounds that are not supposed to resonate in the nasal cavity. Hyponasality consists of too little acoustic energy resonating in the nasal cavity on sounds such as “m,” “n,” and “ng,” which are supposed to resonate in the nasal cavity. Cul-de-sac resonance, sometimes called “hot potato voice” is due to acoustic energy becoming trapped in the pharynx, sometimes due to large tonsils. Ideally, evaluators will be able to obtain a combination of structured and unstructured speech tasks. These should include a connected speech sample, sustained vowels, syllable strings of oral consonants and different vowels, syllable strings of nasal consonants and vowels, and words and sentences specifically useful in identifying a resonance disorder. Different rating scales of hypernasality and hyponasality are used, both clinically and in research. In a clinical setting, most speech-language pathologists use an equal-appearing interval scale, rating hypernasality on a scale of 0 to 4, or 0 to 5 of absent, mild, moderate, severe, and profound. Visual analog scales, direct magnitude evaluation, and a visual rate and sort method have all been used in the literature, and may be more sensitive and reliable than the equal-appearing interval method.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


