18 Medial Epicondylar Debridement
Abstract
Surgical intervention for chronic medial epicondylitis (or enthesopathy of the common flexor-pronator mass tendon origin) is an uncommon end point in the treatment of this largely selflimiting overuse condition. In the rare circumstance where surgery is indicated, several debridement options exist. Macroscopic identification of the pathologic tissue to be removed is not always obvious. “Controlled trauma” to the tendon origin combined with adequate postoperative rest may effectively stimulate or “reset” the dormant reparative pathways and lead to a satisfactory clinical outcome in recalcitrant cases. Addressing concomitant ulnar neuropathy is critical to achieving the best long-term results of upper extremity function.
18.1 Background
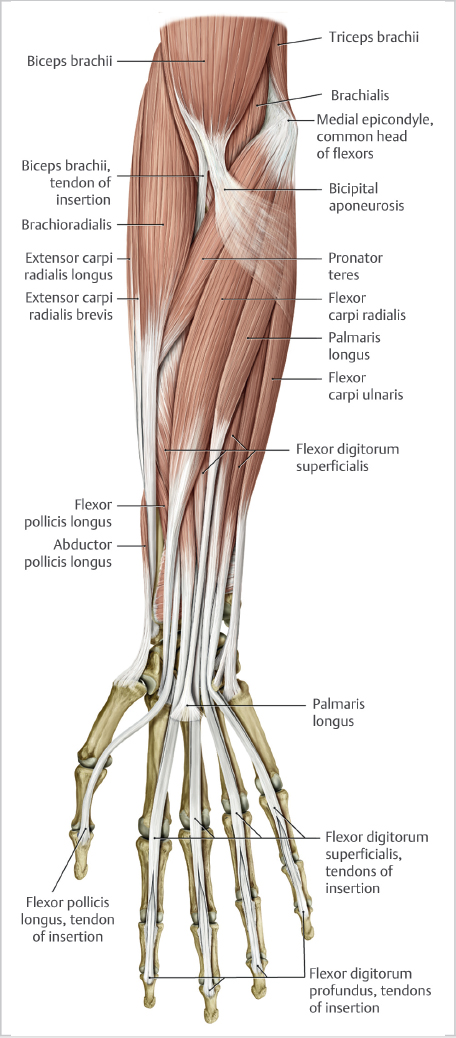
Medial epicondylitis (or enthesopathy of the common flexorpronator mass tendon origin) is a common cause of medial elbow pain (► Fig. 18.1). Surgery to address chronic medial epicondylitis is an atypical treatment end point. Although many conservative strategies can be used for symptomatic patients, there is widespread consensus that the majority of these often middle-aged individuals are not cured by any particular active treatment but rather experience spontaneous symptom decline over a time frame of months to years. Education that emphasizes the avoidance of aggravating activities that correlate directly with symptom exacerbation may be the true cornerstone of treatment and a foundation for a more predictable trajectory of improvement and resolution. Superimposed on this anti- interventionalist thinking is the onslaught of behavioral research shedding light on the interplay between subjective symptom description and psychosocial factors. Periodically, however, there are scenarios where the severity of pain escalates and persists beyond a given individual’s ability to cope, prompting consideration of operative intervention, especially when the symptoms legitimately impact work productivity, jeopardize occupational safety or restrict specific recreational enjoyment. Still, only 26 patients with 2 years of follow-up could be found by investigators at the Mayo Clinic over a near quarter-century review of their operative cases for medial epicondylitis, highlighting the relative infrequency that surgery is indicated. 1
18.2 Pathophysiology
Understanding the pathophysiology of this overuse condition is paramount to crafting the type of surgery required to promote a satisfactory outcome. There has been a scientifically driven shift away from describing the pathologic common flexor pronator tendon origin as inflammatory to recognizing its purely degenerative nature. In fact, the hallmark histologic feature is angiofibroblastic hyperplasia, a term similarly acknowledged in the more commonly seen counterpart of lateral epicondylitis, or enthesopathy of the common extensor tendon origin. This denotes disorganization of collagen composition from a constellation of misplaced metabolic and cellular components. Consequently, the normal healing pathway is thwarted, and the degenerative tissue matrix can neither withstand repetitive forceful wrist flexion/forearm pronation nor the tensile strains on the affected area, thus leading to the subjective experience of pain and weakness. Routine actions such as swinging an axe, throwing a ball, or swinging a golf club become increasingly agonizing and resistant to simple behavioral modifications.
18.3 Evaluation
The overarching reason that surgery may prove successful lies in the concept of “controlled trauma.” Patients often carry a misconception that their elbow tendons are torn or ruptured, often reinforced by the inaccurate language of radiologists interpreting abnormalities at the flexor pronator mass tendon origin on magnetic resonance images. At best, the tendon origin may sustain a cascade of microtears as the genesis of the condition and then functionally deteriorate from the faulty reparative process. Patients must often be convinced that the suggestion of “repairing” this injury is largely misguided. It would be more accurate to introduce and endorse the idea of “intentional collagen regeneration” by surgical means. Simply stated for the layman, this is effectively like hitting an imaginary reset button or creating order out of chaos. Contrasting this endeavor with the example of distal biceps tendon reattachment at its insertion for an acute eccentric rupture may suffice to illustrate the point. Additional reinforcement comes from the lack of noticeable external evidence of tendon disconnection in those afflicted with chronic elbow enthesopathy. This is not to suggest that a traumatic avulsion of the tendon origin isn’t possible, although the forces responsible in that instance would be arguably much larger and often produce simultaneous injury to the skeleton, ligamentous restraints and joint capsule.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


