18 Management of Double-Eyelid Surgery Complications
Pearls
Identify and find ways to avoid the original mistake. Otherwise, secondary and tertiary operations will only compound the problem from the first operation.
Railroad scar from delayed removal of stitches should never happen.
Mechanical resistance to folding of the eyelid skin varies from patient to patient. This resistance is evaluated by observing how long a temporary crease stays after using a bougie.
Deeper folds usually accompany high creases, but crease height is not the same as fold depth.
In secondary eyelid operations, the first goal should be deconstruction of layers through release of adhesion and separation of appropriate planes.
The second goal is the prevention of further complications.
The third goal is to create the desired eyelid shape, including new crease height and fold depth.
The problem behind pretarsal fullness is in the height (not the volume) of the pretarsal compartment. Rather than removing soft tissue, the high crease should be replaced with a lower one.
It is the surgeon’s job to help the patient understand that there is no way to remove an eyelid crease and make the eyes look like their original forms. A better solution is to lower the crease to the eyelid margin and to bury the incision scar within the fold.
Introduction
Aesthetic standards for eyelids vary across ethnic groups and cultures. While a certain contemporary aesthetic standard may be satisfactory to a large number of patients, complications after doubleeyelid operations are specific to the individual patient. Therefore, the authors believe that an outcome that fails to meet realistic patient expectations qualifies as a practical definition for a complication of an aesthetic operation.
In the context of East Asian blepharoplasty, the most common complications are problems of crease height (low versus high), fold depth (shallow versus deep), extraneous creases (triple folds), pretarsal fullness, ptosis, and asymmetry arising from any number of previous conditions.1 This chapter will identify the mistake or the problem behind each complication and present the solution the senior author has developed over his career as an oculoplastic surgeon.
Patient Evaluation
Proper operation depends on proper indication. And proper indication originates from proper diagnosis. In each new preoperative consultation, the surgeon must understand the course of events that prompted the patient to seek further surgical treatment. This understanding comes only if the patient is given ample opportunities to tell the story. Physical examination must correlate with the history. Any discrepancies between the story and physical finding should serve as a warning, and the surgeon must perform due diligence in attempting to rediscover pertinent aspects of the patient’s medical and surgical history.
More often than not, the patient with an unsatisfactory outcome will have multiple complaints. In assessing and counseling the patient, the surgeon must try to offer the ideal operation, which is the one that addresses all of these complaints at once. If no such operation is possible, the surgeon must then offer the optimal solution, which will address as many of the problems as possible at once. For example, a patient may present with a high crease, deep fold, and excessive pretarsal fullness of the upper eyelid. If the surgeon understands that both deep fold and pretarsal fullness are intrinsically tied to the problem of high crease, he or she can appreciate that all three of the problems may be solved by a single procedure: lower the crease.2
Once the simplest solution has been identified, the surgeon must share this information. The patient should understand that the intention is to improve all of the undesirable features to an acceptable degree, rather than to completely solve only a small fraction of the problems. If the surgeon can offer an approach and the patient accepts it, meeting the expectation becomes a mere problem of technicality.
Surgical Techniques
Scar
Eyelid skin does not develop hypertrophic response in most cases. When hypertrophic response is observed after an eyelid operation, the fundamental problem could be the patient’s tendency to develop hypertrophic scar. In many instances, however, the problem is not with the patient but with the surgeon who performed the index operation.
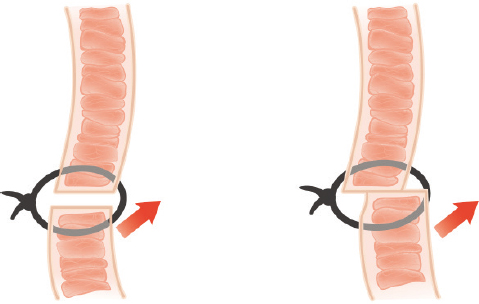
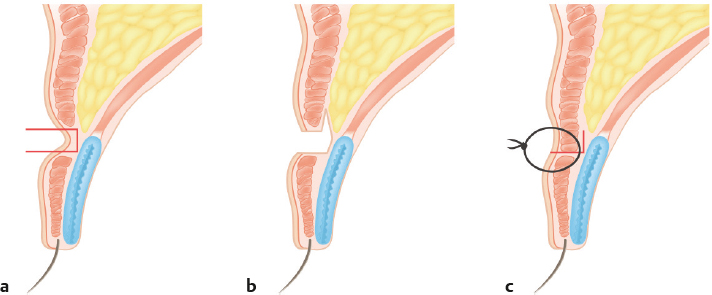
The most common technical mistake is a lack of understanding of the distribution of the superior-posterior force vector of the levator muscle. If this vector is unequally distributed to the lower flap, it is possible to dislocate the lower flap from the upper flap (Fig. 18.1). This occurs more frequently in the lateral portion of the upper eyelid because the aponeurosis is deeper in the tissue. To minimize such a risk, the surgeon must ensure that the upward pull of the levator is transferred to the tarsus—not the skin—via a sufficient number of bites of the plate. In younger patients, skin excisions do not have to be extended along the full length of the eyelid to create a crease of desirable length; a shorter incision design is usually sufficient. A less technical but still common mistake is leaving sutures in for more than 5 days; epithelial tunnels form around sutures only 7 days after operation. Railroad track scars from delayed suture removal are unacceptable. Eyelid scars are more noticeable when they are depressed. Such scars result from excessive removal of the orbicularis muscle, connective tissue (Fig. 18.2), or deep fold (Fig. 18.3).3,4


An eyelid scar revision must obey the wound healing principles that govern all aspects of surgical care. The operation must be aseptically possible. Both surgeon and instrument must be atraumatic with respect to the eyelid tissues. All layers—not just skin—should be approximated with as little tension as possible.
Excision and re-approximation of the skin does nothing to address scars that are depressed. The missing layer of orbicularis oculi must be reconstructed by undermining and advancing the muscle edges from both upper and lower flaps. Such undermining is also beneficial if the problem is that the skin adjacent to the preexisting scar is inverted. When appropriate, undermining of the skin flaps significantly mitigates the tension placed directly across the dermis (Fig. 18.4). Simple continuous suture can place diagonal tension across the wound. An interlocking continuous suture will maintain an even perpendicular tension.
Inclusion cysts result from a prolonged foreign body reaction to the suture placed between the upper and lower skin flaps or from sebaceous gland activity. These cysts may develop over weeks to months after an operation and should be excised if they do not resolve spontaneously (Fig. 18.5). Inclusion cysts are best avoided by using the orbicularis muscle—not the dermis itself—as the anchoring point for the sutures.
Loss of Fold
All surgically created eyelid creases attenuate during the first few months. This change might be minimal, or the fold might disappear altogether. The degree to which a postoperative fold softens is determined by patient characteristics and surgical technique.
The patient-related factors that promote softening or loss of crease are as follows: (1) thick skin and abundant soft tissue, (2) blepharoptosis, (3) sunken eyelid, (4) enophthalmos, (5) history of failed doubleeyelid operation, (6) younger age, (7) low-lying preoperative crease, (8) presence of epicanthal fold, and (9) extreme weight gain. Operative factors associated with technical failure are as follows: (1) inaccurate approximation of connective tissue, (2) insufficient fixation to tarsal plate, (3) low-set fixation, and (4) loosening of the fixation due to hematoma or edema.
Inadequate soft tissue removal along the top margin of the tarsal plate can prevent close approximation of the connective tissue as well as bunching of fat tissue into the loop of the suture. Fat tissue within the loop can introduce mechanical redundancy with expansion from edema and/or hematoma and subsequent disappearance of the surgically created crease.
Although the importance of sutures cannot be overemphasized, a fine distinction must be made between a strong fixation and a proper fixation. A surgically created eyelid fold is a consequence of the adhesion between the anterior and posterior lamellae. Postoperative folds soften and/or disappear over time because the repetitive movement and shifting of various layers are enough to disrupt this adhesion between the layers. To prevent such changes, the adhesions—not the suture material—must be stronger.4
The resistance of an eyelid against forming a fold is estimated during the preoperative consultation. Fold-resistant eyelids tend to require significantly more force when using the stylus, and the created fold disappears rather quickly compared with the eyelids, which maintain postoperative creases without significant changes. Patient factors that predict high resistance to fold formation include thick skin, abundant soft tissue, blepharoptosis, highly elastic skin in younger patients, sunken eyelids, enophthalmos, history of failed doubleeyelid operation, and adhered lower flap. Eyelids with epicanthal folds show high resistance along the medial side. Though this is not a preoperative patient factor, weight gain in the intermediate postoperative period can precipitate loss of a surgically created fold.
To prevent loss of folds, the surgeon must tie the suture while avoiding the intrusion of soft tissue between the levator aponeurosis and dermis or the orbicularis muscle into the loop. If a patient has fold-resistant eyelids, it is important to create a fold that is deep enough to result in the slightest ectropion that will subside after a short postoperative duration. Excessively deep fixations can result in persistent ectropion, even if the fold becomes shallower over time.
Shallow or Deep Fold
Shallow Fold
At times, there is extraneous fat or connective tissue in the pretarsal space. This is especially common on the medial side of the upper eyelid, where pretarsal fat is abundant. Partial resection of this connective tissue can aid in forming an adhesion. If a patient has blepharoptosis or a definite epicanthal fold, these elements must be dealt with first to reduce fold resistance. Otherwise, a deeper fold is necessary.
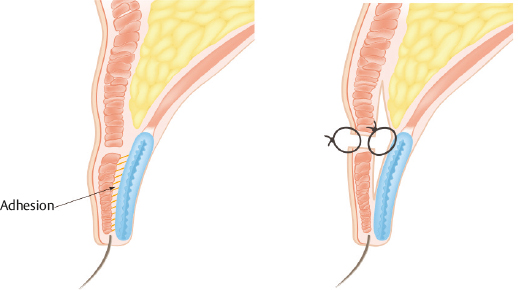
If there is adhesion in the lower flap with softening of the fold, the adhesion will interfere with the formation of a new crease. In such cases, the lower flap must be released and redraped prior to tarsal fixation. In patients whose eyelid skin lacks elasticity after the previous operation, the newly created fold should be deeper than usual to prevent a repetitive loss of fold (Fig. 18.6).
Deep Folds or Ectropion
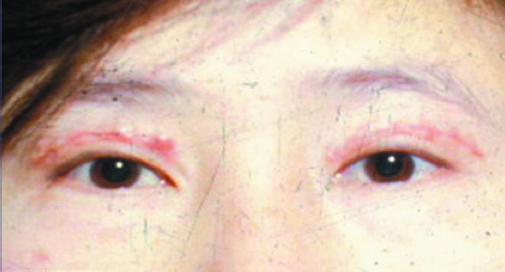
Deep folds and ectropion are caused by creases that were fixated too high on the eyelid. This places an undue upward tension on the lower flap and everts the eyelid margin. A patient often complains about the unintended impression of aggression conveyed by the everted eyelids. The depressed scar is visible when the eyes are closed. The patient may also complain of a tugging sensation in the eyelids. The palpebral fissure may become larger. The skin just superior to the fold tends to bulge.
High fixations inadvertently increase the palpebral fissure because the levator aponeurosis is plicated when the lower flap is fixed at a high point on the levator aponeurosis. In case of severe ectropion, the conjunctiva is exposed. The mucocutaneous junction becomes keratinized, leading to dry eye syndrome.
The first step in correcting the deep fold is to release the adhesions and re-approximate the layers at a lower point along the eyelid. If this part of the operation does not resolve the ectropion, the lower flap must be undermined and redraped over the tarsal plate to decrease the everting force of the adhesion in the lower flap. The second portion of the operation is to prevent the formation of triple folds. The surgeon must take care not to allow readhesion by introducing the orbital fat into the space between the aponeurosis and orbicularis muscle.
Deep crease is often accompanied by a high fold, and the operations to correct these two features are very similar. The only significant difference between the two correction methods is that the location of the previous crease is maintained in cases of deep crease without high fold, the new crease is designed lower than the previous crease, and the skin in between is excised in cases of high fold alone. Correction of deep crease will be described again along with correction of high fold in the following section.
Low Crease
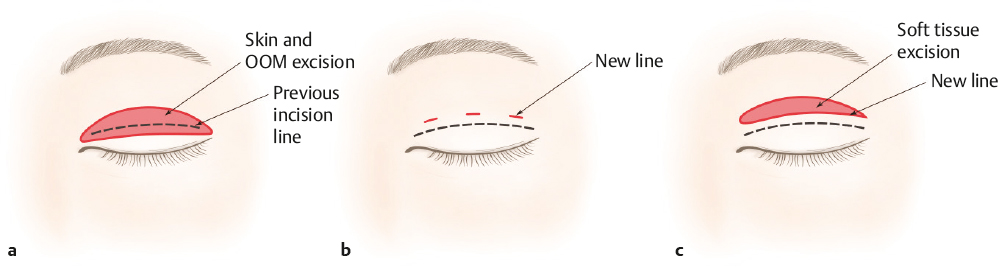
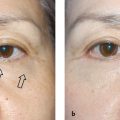
In a crease that is too low, very little skin will show between the eyelid margin and the crease. This is usually a problem of the actual crease design being too low, but a shallow fold can sometimes give the appearance of a low crease (Fig. 18.7). Redundancy of skin can also make a crease appear lower than it really is.

There are three approaches to correct a low fold. The first is an open blepharoplasty by which the skin and orbicularis muscle are excised above the previous crease. The second approach is to create a mechanically overriding crease above the previous one. The third combines soft tissue excision and mechanical fixation above the prior crease (Fig. 18.8).4
The first approach (open blepharoplasty) can incorporate scar revision and allows for excision of redundant skin in older patients. However, the surgeon must leave enough eyelid skin to minimize the risk of postblepharoplasty brow ptosis. In patients without significant redundancy of eyelid skin, excision of the orbicularis muscle above the old crease is more important than excision of the skin. Maximum elevation of the eyebrows should result in 80 to 90% elevation of the upper eyelid margin in patients with an appropriate amount of skin excised. This is an important part of the preoperative and intraoperative guideline on estimating how much of the upper eyelid skin is redundant.
The second approach (tarsal fixation) allows considerable elevation of the fold crease but will create an additional scar, if secondary incisions are necessary. This approach is more appropriate for patients who have inconspicuous scars from the first operation and wish for the eyelid fold to be higher. If the previous fold is strongly defined (i.e., too deep), then a simple mechanical fixation may result in multiple eyelid folds. To minimize such risk, the lower flap can be undermined through a small incision window. This can significantly attenuate the primary fold to a faint appearance. Patients should be warned of the potential for pretarsal fullness from the scar tissue after the initial operation.
The combined approach of open blepharoplasty and mechanical fixation is reserved for patients with very low folds and great redundancy of skin.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


