15 Epicanthoplasty and Aesthetic Lateral Canthoplasty
Pearls
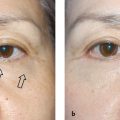
Cosmetic epicanthoplasty releases the epicanthal fold and modifies the medial corner of the palpebral fissure, thus revealing more of the medial portion of the eye and decreasing the interepicanthal distance.
The lacrimal caruncle can be triangular, round, or hook-shaped, and these variations need to be considered in selecting an approach for epicanthoplasty.
When modifying the canthus for aesthetic reasons, a conservative approach is recommended because an over-corrected epicanthus is extremely difficult to revise.
Right and left lacrimal caruncles have different scales of growth and direction, which needs consideration in the design of epicanthoplasty.
When a doublefold operation is combined with epicanthoplasty, redundant skin from the upper flap of the double eyelid should be rotated toward the deficient skin on the inner part of the lower eyelid to decrease the risk of partial ectropion.
The two most frequent complications of epicanthoplasty are scarring and the aggravation of the epicanthus inversus. These risks can be reduced by designing the skin incisions along the relaxed skin tension lines and avoiding a connection between the epicanthoplasty and blepharoplasty incisions.
In aesthetic lateral canthoplasty, not only horizontal palpebral extension but also proper posterior deepening is important to maintain a proper contact between the eyeball and palpebral conjunctiva.
Combined lateral canthoplasty and lowering of lower eyelid slant will make the eyes look mild and big. Mongolian slant lowering can be done by suturing between the tarsus and capsulopalpebral fascia.
Epicanthoplasty
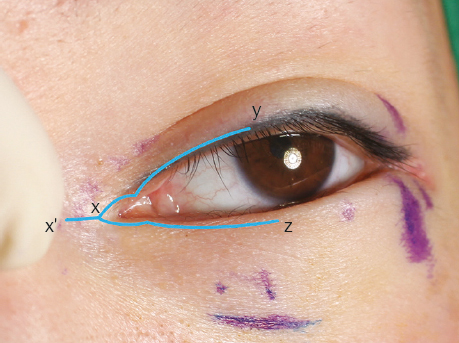
The epicanthal fold is excessive fibrous tissue that lies in a vertical, semilunar orientation, and it is a distinctive feature of the Asian eyelid. Cosmetic epicanthoplasty releases the epicanthal fold and modifies the medial corner of the palpebral fissure. The operation reveals more of the medial portion of the eye while simultaneously decreasing the interepicanthal distance (Fig. 15.1).
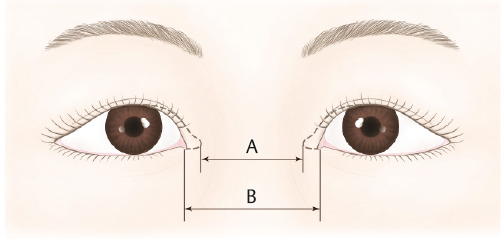
In East Asian populations, the mean interepicanthal distance is reported to be 3.48 to 3.6 cm.1 Among beauty contestants in the 2003 “Miss Korea” contest, this distance was 3.17 cm on average, which is shorter than the mean value, and this implies that the contestants probably did not have highly conspicuous epicanthal folds. The interepicanthal distance should be interpreted in the context of the overall relationship between the epicanthal fold and the remainder of the eye. Epicanthal folds appear most natural when less than half of the caruncle is covered. Usually, 80 to 90% exposure of the caruncle is aesthetically pleasing.1,2
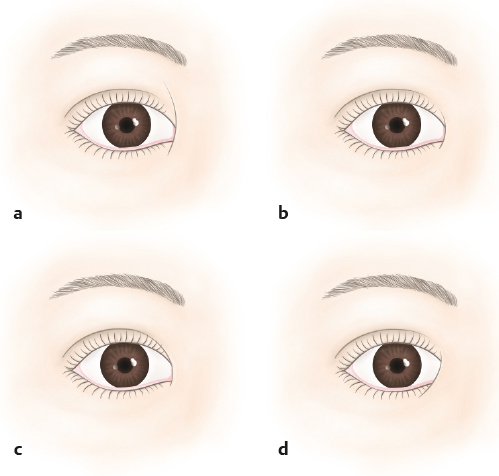
The shape of the lacrimal caruncle can be triangular, round, or hook-shaped. Triangular caruncles account for 53% and are mostly found among Asian patients. The round caruncles represent ~ 10%. The hook shape (37%) is accompanied by a down-pointing medial palpebral commissure (Fig. 15.2).3

For triangular and round caruncles, the extent of epicanthal release is determined considering the whole proportion of the eyes. However, hook-shaped caruncles require a different approach because epicanthal tendons run downward along the outer curvature. If too much of this epicanthal fold is eliminated, the outcome will be an aggressive appearance that will most likely to be unacceptable to the patient. The size of visible caruncle after epicanthoplasty is an important consideration. In East Asian patients, the caruncle is visible for 3 to 5 mm at the medial side. If the epicanthal fold covers the caruncle and the externally visible part of the caruncle is 1 mm or less, a more drastic intervention may be required.
Epicanthal folds can be divided into four types: epicanthus supraciliaris, epicanthus palpebralis, epicanthus tarsalis, and epicanthus inversus (Fig. 15.3).1 Epicanthal folds represent a wide spectrum of soft tissue configurations with varying etiologies, and thus there cannot be a single operation that is suited for all patients and situations. The sheer numbers and variations of epicanthoplasty techniques serve to demonstrate this fundamental concept in epicanthoplasty.
Early in its development, epicanthoplasty consisted only of skin excision with the idea that epicanthal folds were manifestations of redundant skin around the medial canthus. However, a common complication of this method was visible scarring caused by excessive tension in the skin, especially in the lower one-third of the medial canthus. On one hand, skin redundancy in the upper third of the epicanthal fold is usually accompanied by a skin deficiency of the lower third. In such configuration, the redundant skin should be used as a flap to relieve the tension on the lower third, which is crucial in the prevention of ectropion along the medial portion of the lower eyelid. On the other hand, skin redundancy of the lower section indicates that the epicanthal fold is caused by multiple factors. Even if the lower skin is not deficient, upper excessive skin excision should be minimized in such cases.
Patient Evaluation
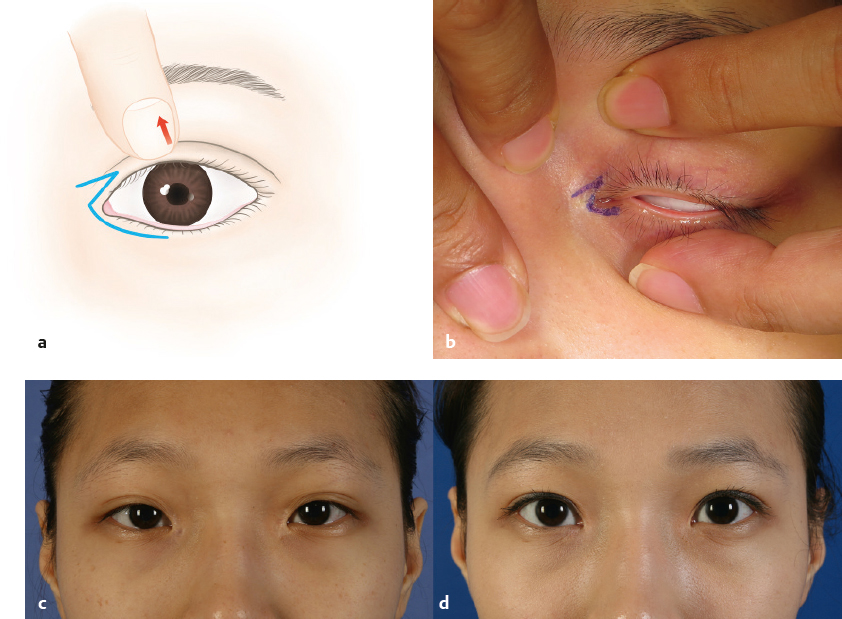
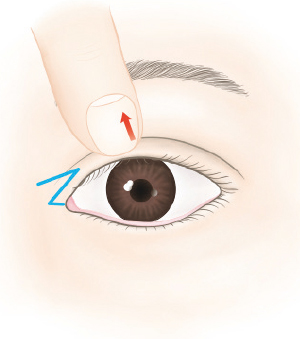
It is important to measure the interepicanthal distance and the amount of exposed lacrimal caruncle. Patients with extreme epicanthal fold and wide interepicanthal distance can realize a dramatic benefit from this procedure. A patient can inspect the changes after epicanthoplasty by finger traction of the inner canthus. Under-correction is safer than overcorrection because an undercorrected epicanthal fold can be revised much more easily than an over-corrected epicanthal fold.
Of the four types of epicanthal folds, epicanthus tarsalis is most common in East Asians. Not all epicanthal folds require correction, and epicanthus tarsalis allows for a more naturallooking epicanthus with double fold. East Asians tend to have thicker skin near the nasal bridge and epicanthal area than in the upper eyelid, which is more reactive and prone to hypertrophic scarring after epicanthoplasty. Preoperatively, patients should always be informed that undercorrected or asymmetric epicanthus may develop as a complication.
Each epicanthal fold can be divided into upper, middle, and lower thirds. For each portion, anatomic features should be thoroughly examined, such as skin redundancy, extent of skin hooding, and amount of soft tissue tension. Even in a single patient, the sizes of the bilateral lacrimal caruncles may differ, so the side of the smaller caruncle should be opened more widely to make for symmetry after epicanthoplasty. Therefore, it is crucial to prepare a precise medical examination and diagnosis.
Double-Fold Operation and Epicanthoplasty
In East Asian patients, the doublefold operation is commonly performed in conjunction with epicanthoplasty. In such a combined operation, the redundant skin from the upper flap of the double eyelid should be rotated toward the deficient skin on the inner part of the lower eyelid. This redistribution of soft tissue is helpful in decreasing the risk of partial ectropion caused by epicanthoplasty (Fig. 15.4).
If epicanthoplasty is performed without the doublefold operation, a dog-ear might form on the upper and medial parts of the epicanthal fold and will need excision. Occasionally, this excision can result in a new, unwanted doubleeyelid line. To prevent this new doubleeyelid line, the dog-ear should be resected as close to the upper cilia as possible. If the skin is insufficient on the lid margin of the medial caruncle, the dog-ear portion of the upper flap should be preserved and turned into a triangular flap to be rotated into the inner portion of the new canthotomy structure (Fig. 15.5). Another possibility is to release the band-shaped epicanthus inversus on the lower part of the epicanthal fold by rotating the flap made by the dog-ear and advancing the triangular flap perpendicularly to the epicanthus inversus.
Surgical Techniques
There is no single technique that can address the full spectrum of epicanthal folds, and the surgeon must rely on a set of techniques that are applicable to specific types of epicanthal folds. Most epicanthoplasty techniques are variations and combinations of a few fundamental concepts: simple skin excision, V-Y advancement, Z-plasty, and W-plasty. The following five questions must be answered before the appropriate epicanthoplasty technique can be chosen.
How will I manage the skin redundancy and deficiency?
How will I control the extent of caruncle exposure?
Can the transverse incision be placed in a nonvisible area or along a relaxed skin tension line?
Is it possible to leave a skin bridge between the epicanthoplasty incision and the doubleeyelid incision?
Of the appropriate operative techniques, which am I most comfortable with?
Simple Skin Excision
Simple skin excision is not complicated and can be performed even by inexperienced surgeons. Although skin-only excision can be suitable for some cases, excessive tension in the lower flap is a concern and can result in postoperative scarring. To decrease tension, the soft tissue must be dissected and the perpendicular accessory fiber must be transected. This method is not commonly performed nowadays.
V-Y Advancement Methods
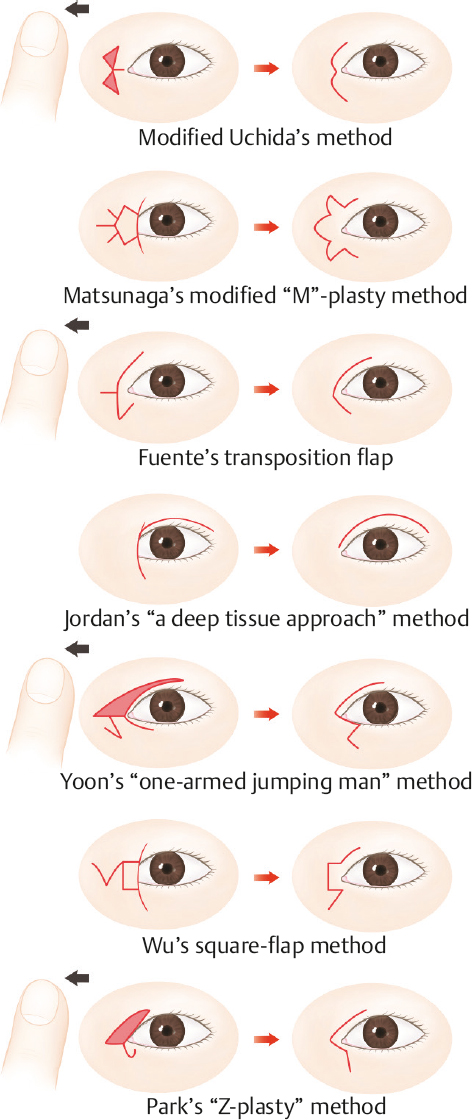
There are several known variations of V-Y advancement. The Roveda method involves advancement of the nasal side skin and removal of the remaining skin from the top and bottom to prevent dog-ear. Uchida modified the Roveda method, but the Uchida design was too close to the lacrimal caruncle to prevent noticeable scars. The Uchida method has been further modified to the periciliary epicanthal fold incision method, which involves a large V-shaped incision followed by dissection and excision of the surrounding skin to completely hide the scar (Fig. 15.6).4
Z-Plasty Flap
This is a frequently used technique with many variations to allow for flexibility in the location and size of the two skin flaps. Fuente’s design incorporates half of a Z-plasty, which takes the triangular flap from the lower part of the epicanthal fold and transfers it to the middle part, and extends the doubleeyelid fold incision line toward the inner upper part. This method is recommended for patients with a preexisting doubleeyelid fold. However, resection of redundant skin is necessary, if the technique is performed simultaneously with the doublefold line operation (Fig. 15.7).
Park’s method is a modification of Fuente’s method and incorporates partial resection of redundant skin between the doubleeyelid fold line and the epicanthoplasty site. This method rotates skin from the lower epicanthal fold to the middle portion. The redundant skin in the upper epicanthal fold is resected. This procedure is suitable for patients who have the redundant skin in the lower epicanthal fold with high tension in the middle portion. The technique is also useful in addressing the dog-ear from the redundant skin along the upper blepharoplasty incision line.
The reverse design of Fuente’s method can be used for patients with redundant skin on the upper part of the epicanthal fold and lack of skin on the lower part. In such cases, the triangular flap should be made on the upper inner part and rotated downward (Fig. 15.4). If less than 1 mm of lacrimal caruncle is visible, then the triangular flap from the upper part of the epicanthal fold is rotated into the medial canthotomy site (Fig. 15.5).
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


