14 Aging-Related Upper Blepharoplasty
Pearls
Understanding anatomic differences and involutional changes in the eyelids of East Asians, which are specific to age and gender, is the key to achieving optimal results.
Too much is as unwelcome as too little. The trend in Asian aging-related blepharoplasty is toward conservative excision of skin and fat, making a naturallooking, low-positioned double eyelid (or not making an artificial double eyelid).
It is important to have a realistic understanding of the outcome of blepharoplasty through an in-depth discussion between the surgeon and the patient before surgery. The goal of aging-related blepharoplasty is to restore the individual’s youthful appearance while retaining the ethnic characteristics. This is especially true in the case of treating the Asian upper eyelid.
The upper crease is usually low or absent in the Asian eyelid. Slightly folded upper eyelid skin over the doubleeyelid crease, or a low doubleeyelid crease (e.g., 3–4 mm in height) looks more natural and blends well. Usually, a doubleeyelid crease over 7 to 8 mm in height looks very unnatural in Asians, even in female patients.
Brow ptosis usually occurs after middle age, and dermatochalasis and blepharoptosis may appear accentuated due to brow ptosis. Therefore, the surgeon must recognize brow ptosis before surgery and decide whether to perform a brow lift in advance or do it in conjunction with the blepharoplasty.
Many aged people who want blepharoplasty may have blepharoptosis of some degree but may not be aware of it because it is concealed by the dermatochalasis.
If the patient complains of ocular irritation symptoms, problems with tear secretion such as dry eye syndrome could be present. The surgeon should make the patient understand that ocular irritation may be aggravated after blepharoplasty and that such problems need to be managed before blepharoplasty.
The most difficult cases of aging-related blepharoplasty in Asians involve patients who had undergone previous blepharoplasty with excessive skin and fat removal, with a very high-positioned doubleeyelid crease. In these cases, autologous fat or filler injection along the brow and upper eyelid complex is more helpful in improving the cosmetic outcome than a blepharoplasty.
The lacrimal gland is located laterally just behind the orbital rim, and normally it is not seen during blepharoplasty. With aging it prolapses, which might be mistaken for lateral fat prolapse, especially in Asian patients who have thick skin over the lacrimal gland.
Complications after aging-related blepharoplasty are usually the result of excessive skin or fat resection, lack of hemostasis, an inadequate preoperative assessment, or careless postoperative management. Every effort should be made to minimize or prevent complications during or after blepharoplasty by recognizing known risk factors and paying careful attention during and after surgery.
Introduction
East Asians are the world’s largest ethnic group, and the eyelids’ position in the center of the face is a distinguishing feature and makes a strong impression. Blepharoplasty is the most common and a rapidly growing cosmetic surgery procedure in Asia. Understanding anatomic differences related to eyelid surgery is the key to achieving optimal results. A typical Asian eyelid is a single eyelid with an epicanthal fold or Mongoloid slant. Improving a patient’s appearance while maintaining the person’s ethnic characteristics is the goal of Asian eyelid surgery.1 The goal of aging-related blepharoplasty is to restore the individual’s youthful appearance, not to create a morphologic change that brings a novel look. This is especially true in the case of treating the Asian upper eyelid. Loss of ethnic identity can result in a negative reaction both from the patient as well as from his or her friends and family.2
In the past it was generally accepted that Asian patients wanted to have double eyelids to project a more Western appearance, which they found more attractive. However, the trend these days in Asian aging-related blepharoplasty is toward conservative excision of skin and fat, giving a naturallooking, low-positioned double eyelid and not creating an artificial-appearing double eyelid. Nowadays most aging Asian patients want to restore their youthful appearance but at the same time retain their ethnic characteristics, not Westernize their eyelids, through blepharoplasty surgery.
Periorbital changes with aging include dermatochalasis, crow’s feet, and periorbital fat prolapse, and these lead to changes in eyelid contour. The goal of blepharoplasty in aging patients is to correct these processes and to allow the patient to look younger. Blepharoplasty in elderly people is mostly incisional blepharoplasty. To improve the periorbital wrinkles or superior hollowness, filler or botulinum toxin injections may follow. Periorbital change with aging is a dynamic process involving the aging of facial tissue and bony structures, and several changes are common. Epidermal thinning and decreased collagen cause the skin to lose its elasticity. Loss of fat, coupled with gravity and muscle pull, leads to wrinkling and the formation of dynamic lines. The aging process has also been shown to affect facial bones. Multiple studies suggest that bone aging of the orbit and midface occur primarily due to contraction and morphologic changes. This loss of bony volume and projection may contribute to the aged appearance. The effort to understand each patient’s individual involutional changes, which are specific to age and gender, is mandatory. Therefore, identifying the patient’s personal needs and selecting the right treatment accordingly is crucial for achieving the best outcome both for the clinician and for the patient.3
The eyelid is important not only in its functional aspects such as tear distribution from blinking, but also in its cosmetic aspects because it greatly affects other people’s impressions by defining one’s facial characteristics. The drooped brow and eyelid skin can obscure one’s view and look heavy, and lateral eyelid skin can be folded and thus cause eczema.4 The eyelid becomes puffy due to the prolapse of orbital fat from the loosening of the orbital septum.
Blepharoptosis refers to drooping or infratransposition of the upper lid. The most common type of acquired ptosis results from stretching or weakening of the levator palpebralis due to involutional change or disinsertion of the levator aponeurosis from the tarsal plate. It causes not only cosmetic problems but also visual discomfort such as obscuring the view. Although the superior visual field is primarily involved, many patients complain of difficulty with reading because the ptosis is aggravated with down-gazing. Park et al reported that Koreans age 50 years or older showed a very high frequency (54.9%) of ptosis, and as the age increases, the frequency of ptosis also increases.5 The examiner should note the patient’s head position, chin-up position, or brow position to detect the presence of ptosis.
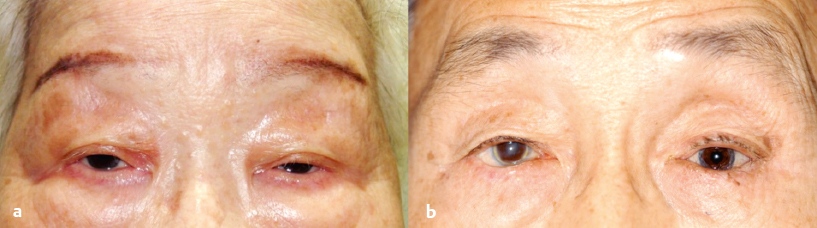
Patients often involuntarily attempt to compensate for dermatochalasis by chronic use of the frontalis muscle and this can lead to high-positioned eyebrow and deep (prominent) transverse furrows in the forehead (Fig. 14.1). Unlike other areas of the body, where there is descent of soft tissues, there may be paradoxical elevation of eyebrows with aging, especially the medial and midbrow. So the clinician should try to determine the eyebrow morphology and position of the individual patient and selectively elevate the lateral brow to have a rejuvenating effect on the upper third of the female face.6
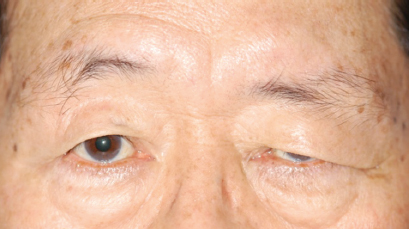
On the other hand, brow ptosis frequently accompanies dermatochalasis, and the patient can be over-diagnosed as having very severe drooping of the upper eyelid skin and excessive excision of skin with subsequent further dragging of the eyebrow downward. Therefore, the examiner should check for any history of facial nerve palsy in case of unilateral brow ptosis (Fig. 14.2). Seo and Ahn analyzed the morphologic changes of the eyelid according to gender among different age groups in Koreans and reported that the degree of brow ptosis showed a statistically significant increase from the seventh decade of life in men and from the sixth decade in women. In particular, the lateral brow drooped more than the center brow. The lateral hood width of the eyelid showed a statistically significant increase from the seventh decade of life in men and from the sixth decade in women.7
Patient Evaluation
Dermatochalasis
Elderly people commonly complain of “blepharoptosis,” but most cases are not real ptosis but rather dermatochalasis: simple skin and muscle drooping. To distinguish real ptosis from simple dermatochalasis, raise the drooped skin and check the position of the eyelid margin. Patients with simple dermatochalasis show normal eyelid height similar to that of young people, and those cases usually need excision of the skin and muscle only.
Deep Superior Sulcus
The dehiscence of the levator aponeurosis from the upper tarsal plate can cause high placement of multiple creases and hollow superior sulcus (Fig. 14.3). Dehiscence of the levator also causes ptosis, and subsequent brow elevation to compensate for this ptosis can aggravate superior sulcus deepening.8,9 Sometimes previous excessive fat removal may cause a deep and hollow superior sulcus with involutional changes.

The Degree of Blepharoptosis and Levator Function
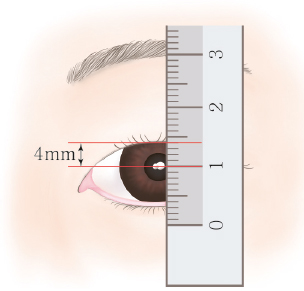
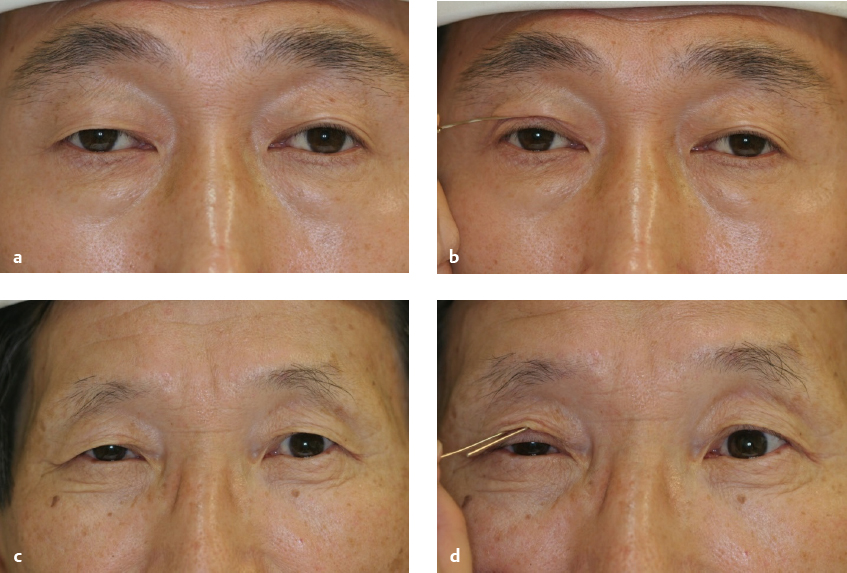
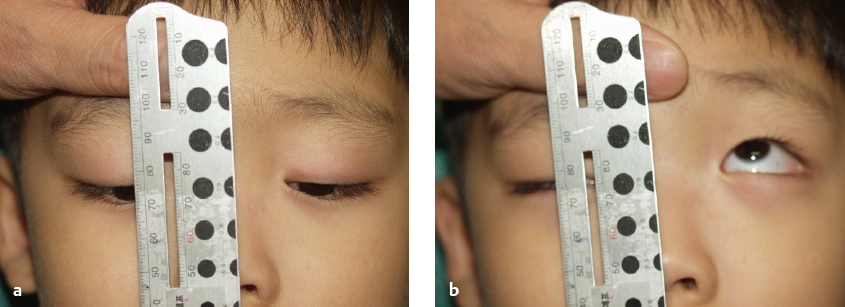
Many aged people who want blepharoplasty may have blepharoptosis of varying degrees. To check the degree of blepharoptosis and levator function, the patient should stay comfortable and should not use the frontalis muscle. First, examine whether the position of the lower lid is normal. Second, check the margin-reflex distance (MRD), the distance from the upper eyelid margin to the corneal light reflex in the primary position, which is the most effective measurement in describing the amount of blepharoptosis (Fig. 14.4). Patients with severe dermatochalasis may also have blepharoptosis; however, these patients can be overlooked because dermatochalasis can conceal their blepharoptosis. The most simple and effective way to find hidden blepharoptosis is to curl up redundant skin and find the real MRD from the eyelid margin to the reflex, not the manifest MRD, from the skin margin to the reflex (Fig. 14.5).
Third, measure the levator function by determining the distance (in millimeters) the upper eyelid margin moves from down-gaze to up-gaze while the brow is fixated with the examiner’s fingers (Fig. 14.6). Decreased lifting force might also explain lash ptosis, which is not only present in the single eyelid but also increases in prevalence in the double eyelid with aging.10 The degree of lash ptosis correlates with the degree of blepharoptosis and decreased lifting force of the levator aponeurosis.11
Brow Position
The brow is normally positioned at the level of the superior orbital rim, and the male brow is lower than the female brow. Brow position and contour determine youthful appearance to some degree. With aging, the temporal brow starts to droop more prominently because the frontalis muscle is not present in the lateral brow area. Drooping of the brow is called brow ptosis. Brow ptosis occurs usually after middle age, and dermatochalasis and blepharoptosis may appear accentuated due to brow ptosis. The surgeon must recognize the brow ptosis accompanying dermatochalasis as a contributing factor in the patient’s aged appearance before surgery. In the presence of brow ptosis, the surgeon must decide whether to perform a brow lift in advance or in conjunction with the blepharoplasty. The medical history must be checked for facial nerve palsy in cases of unilateral brow ptosis or more prominent drooping of the unilateral upper eyelid skin. If brow ptosis was overlooked, iatrogenic postoperative lagophthalmos can result from the resection of too much skin and muscle. Therefore, to get good results, the brow lift has to precede blepharoplasty.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


