12 Double-Eyelid Surgery: Nonincisional Suture Techniques
Pearls
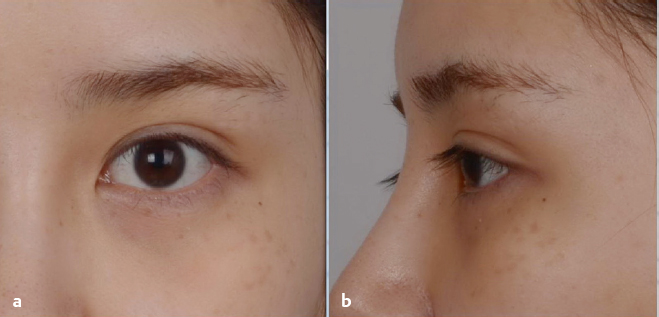
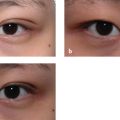
The pattern of skin fold formation in the opening phase of the upper eyelid is characteristic of the East Asian individual. In a double eyelid, the upper border of the eye consists of two outlines, as if the upper eyelid were composed of dual layers.
The creation of an artificial connection of skin (anterior lamella) and levator (posterior lamella) at a higher level is the main feature of the doubleeyelid procedure.
Nonincisional suture ligation creates a fold without dissection. It is a simple, noninvasive, and efficient technique to make a double fold, but it has also many contraindications. For example, revision blepharoplasty is performed to reduce the height of the fold, especially after a previous incisional blepharoplasty.
The nonincisional suture technique needs to be modified considering various factors such as puffy eyelid, weak levator function, and exophthalmos. For a puffy eyelid, the septal fat should be removed as much as possible, and the new crease line designed to be as low as possible. Too high a fold may hinder the full opening of the aperture and yield opening discomfort, especially in a subclinical or clinical ptotic eyelid. If exophthalmos is prominent, the line of the crease should be lowered more than usual to avoid an excessively high fold.
The lid margin may be closed (“inside fold”) or open (“outside fold”) at the medial end according to whether or not the two upper outlines of the eye, the edge of the skin fold, and the true lid margin with the eyelashes are joined together medially.
The middle portion of the double fold should be sufficiently higher than the medial and lateral portions in the closed state to prevent straightening of the double fold when the eyes are open.
After preoperative design, five punctures or small slits should be made with a needle or no. 11 blade. A 7–0 nonabsorbable suture is passed through the skin to the upper margin of the tarsus and returned through the same site of the tarsus to the skin. Then the lid skin is fixed on the tarsal plate.
When removing the septal fat, the position of the fat must be considered. The septal fat moves to an upper and lateral area in the supine position.
For Müller muscle tucking, 7–0 nylon thread is introduced through the skin to the upper margin of the tarsus. The suture is passed through the tarsus to the point of the conjunctiva near the superior fornix and returned through the same point on the conjunctiva to the tarsus, tucking the Müller muscle. The suture exits through the tarsus to the skin and is knotted to tighten the thread.
When the suture passes through the tarsus, the suture may appear on the conjunctival side, which can induce a foreign body sensation and severe pain. If the patient complains of a foreign body sensation, the eyelid is everted and the tarsal plate is carefully scrutinized.
Introduction
Double Eyelid and Single Eyelid
One of the most important functions of the upper eyelid is to alternately protect and expose the eye with its repetitive shutter-like excursion movement. Along with the alternating motion of the closing and opening phases, the upper eyelid changes its external shape continuously. In the closing phase, the lid is extended wide to cover the cornea and bulbar conjunctiva of the eyeball; in the opening phase, the lid is retracted to expose them. During the opening period, the enveloping cover (skin and palpebral conjunctiva) should be folded to eliminate redundancy in temporary coverage. Although conjunctival folding is not observed when looking at the face, the pattern of skin fold formation in the opening phase of the upper eyelid is characteristic of each East Asian individual.1 This pattern and manner of folding the outer skin determines the shape of the eyes, particularly in the upper border of the palpebral aperture. Usually, the skin is folded at the middle of the eyelid, and the edge of the skin fold is located above the eyelash to expose the cornea completely in the fully opened state. The edge of the skin fold and the eyelid margin with the eyelashes parallel to each other form the upper border of the palpebral aperture (double eyelid) together. In a double eyelid, the upper border of the eye consists of two outlines as if the upper eyelid were composed of dual layers (Fig. 12.1).
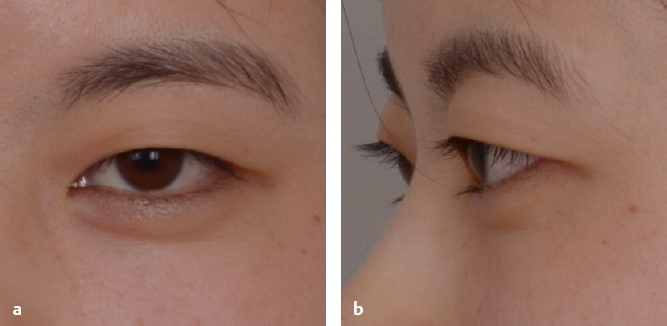
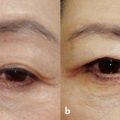
In contrast, the single eyelid has only one border, because the skin fold is formed below the lid margin. The edge of the skin fold hides the real lid margin and pushes the eyelashes from above in the opening phase (Fig. 12.2). Compared with the double eyelid, the palpebral aperture is reduced by the lower skin fold. The single-lined upper border is a unique feature of East Asian individuals (Korean, Chinese, Japanese, and Mongolian), while the double line is the most prominent eyelid fold pattern in Caucasian, African American, and South Asian individuals.
Anatomy of the Upper Eyelid
The upper eyelid is a layered structure, divided into the anterior, middle, and posterior lamellae. The anterior lamella is composed of the skin and underlying orbicularis oculi muscle. The posterior lamella consists of the tarsus and underlying conjunctiva. The middle lamella consists of the orbital septum and fat separating the orbital contents from the preseptal structures.2 In the sagittal sectional anatomy, the inverted triangle-shaped upper eyelid has a thick upper portion with three distinctly separated lamellae and a thin distal lid margin in which the anterior and posterior lamellae are attenuated and condensed firmly together (the skin, orbicularis oculi muscle, and tarsus). The intervening orbital septum and orbital fat (middle lamellae) extend only to the fusion line, which can be identified as a skin crease on the outer surface. The condensed distal lid margin is attached to the levator mechanism (levator aponeurosis, superior levator palpebralis muscle, and Müller muscle) and actively retracts at the beginning of the opening phase (Fig. 12.3). Meanwhile, the anterior and middle lamellae above the fusion line (transverse skin crease) are passively folded according to the opening movement.
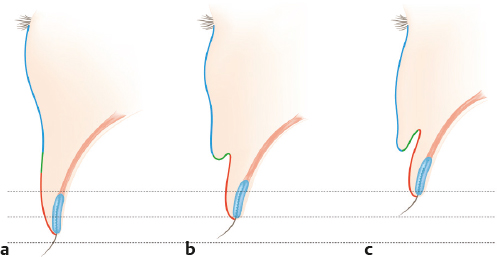
With the superior levator palpebralis muscle contracting, the distal lid margin (red-colored surface) directly connected to the levator mechanism begins to retract upward, leaving the upper anterior lamella (above the fusion line, green- and blue-colored surface) static in situ. As the degree of opening increases, the anterior lamella just above the crease is passively lifted from its distal end (greencolored surface). At this level, the transverse skin crease becomes prominent and is folded further as opening progresses. With further opening, the distal skin of the anterior lamella (green) is flipped up and enters just behind its upper skin (blue-colored surface) to create a fold.
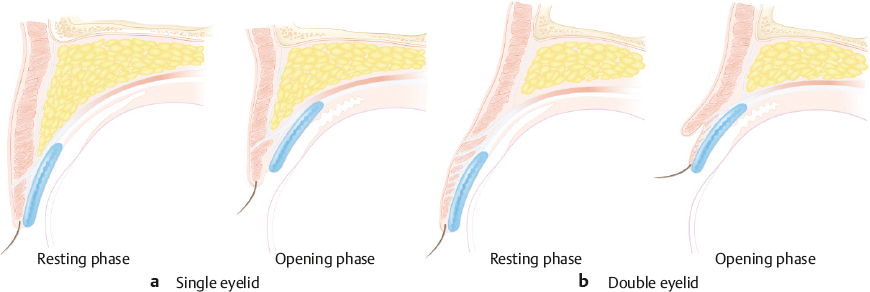
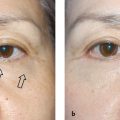
In the single eyelid, the middle lamella is well developed and abundant orbital fat extends to a lower level. Therefore, the anterior and posterior lamellae fuse at a lower level than they do in a double eyelid, and the height of the condensed distal lid margin (red) is too low. As a consequence, the skin of the anterior lamella is folded at a much lower level (lower tarsal crease) in the opening phase and hides the entire lid margin, including the eyelashes. Furthermore, the upper portion of the palpebral aperture is partially eclipsed by the skin fold, despite the full opening of the eyelid. Hence, in a severe case, the frontalis acts to lift the eyelid skin fold to provide adequate vision, as in a patient with a blepharoptosis. Meanwhile, in a double eyelid, the fold is formed at a higher level and the edge of the fold lies above the lid margin and does not obstruct the normal visual field (Fig. 12.4).3,4
Nonincision Suture Ligation for Double-Eyelid Formation
The most important anatomic difference between a single and double eyelid is the level of the lid crease and skin fold formation, which is the result of the thinning and fusion of the anterior and posterior lamellae. In a double eyelid, the skin fold lies within the lid above the eyelash in a relaxed forward gaze, because the fold-forming lid crease is well defined and sufficiently high. The creation of an artificial connection of skin (anterior lamella) and levator (posterior lamella) at a higher level is the main feature of the doubleeyelid procedure.
Traditionally, the procedure can be divided into two major categories: nonincisional suture ligation (buried suture technique) and the external-incision technique. While the nonincisional technique connects the skin and the deeper active levator mechanism with a simple thread loop, the external-incision technique consists of reducing the volume of both lamellae and fixing them together with scar adhesion. The external-incision technique also requires a buried suture to connect the skin and levator mechanism, so a suture loop ligation is common to both techniques. Regardless of the use of an incision, a buried suture loop in the lid is an essential part of doubleeyelid creation. In fact, the nonincision suture ligation technique entails forming a fold with suture ligation without dissection. Various surgical approaches for nonincisional suture ligation have been reported. The nonincision suture ligation technique has been developed for correction of blepharoptosis as well as for the simple formation of the doubleeyelid fold. From the conjunctival side, the retractor can be plicated to increase the tension of the levator mechanism.
Patient Evaluation
With the exception of severe blepharoptosis with weak levator function or extremely thick lid soft tissue, the nonincision suture ligation technique can be applied to transform the lid from single to double in most patients. However, the procedure is selected based on the specific requirements of the case and the anatomic and functional conditions of the patient.
Puffy Eyelid
A stable adhesion of the previously separated anterior and posterior lamellae at a higher level is the primary goal of doubleeyelid surgery. The intervening loose voluminous tissue (orbicularis oculi muscle and preseptal and septal fat) between the skin (anterior lamella) and levator mechanism (posterior lamella) is the main hindrance to the fusion of the lamellae. Hence, excessive soft tissue in the upper eyelid is an unfavorable factor for doubleeyelid formation using either the external-incision or nonincisional suture ligation procedure. While the septal fat can be removed with a small incision before suture ligation (partial incision suture ligation), the preseptal fat and orbicularis oculi muscle cannot be reduced without a full-length incisional technique. For a puffy eyelid, the septal fat should be removed as much as possible, and the new crease line should be designed to be as low as possible in a nonincision suture ligation procedure (strictly speaking, this should be named “partial incision suture ligation” because the fat is removed through a small incision before suture ligation).
Weak Levator Function
Although Müller muscle tucking can resolve mild blepharoptosis, it is contraindicated in most cases of severe blepharoptosis with a loose levator aponeurosis that requires direct levator advancement. The creation of a higher folding crease increases the load of the dynamic part of the lid. Furthermore, the upper portion of eyelid skin is thicker and requires more force to fold. Too high of a fold may hinder the full opening of the aperture and yield opening discomfort, especially in a subclinical or clinical ptotic eyelid.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


